




Pristiq (desvenlafaxine) reduces anxiety symptoms, although it is not FDA-approved for anxiety disorder.
Pristiq inhibits the reuptake of serotonin and norepinephrine in limbic and prefrontal circuits. It is prescribed off-label for managing anxiety. Psychiatrists prescribe desvenlafaxine for generalized anxiety disorder (GAD), social anxiety disorder, and panic disorder when first-line options have failed or caused intolerable side effects.
Understanding how this medication works, how long it takes to act, and how it compares to alternatives helps patients make informed decisions alongside their prescribers.
Key Takeaways
- Pristiq is FDA-approved only for major depressive disorder (MDD) in adults; its use for anxiety is off-label, supported by clinical trials demonstrating efficacy for GAD and social anxiety disorder at the 50 mg/day standard dose.
- Desvenlafaxine inhibits the serotonin transporter (SERT) and norepinephrine transporter (NET) simultaneously, bypassing the CYP2D6 metabolic pathway that complicates venlafaxine dosing in poor metabolizers and patients on CYP2D6-interacting drugs.
- According to the National Institute of Mental Health, anxiety disorders affect approximately 19.1% of U.S. adults annually, making off-label SNRI use a clinically important tool when FDA-approved first-line options produce inadequate response.
- Most patients experience initial anxiolytic effects within 2–4 weeks of starting Pristiq, with full therapeutic response typically requiring 4–8 weeks of consistent dosing at 50 mg/day.
- Pristiq discontinuation syndrome: driven by SERT and NET re-engagement: produces dizziness, brain zaps, and irritability when the drug is stopped abruptly; tapering over several weeks prevents most withdrawal effects.
What Is Pristiq (Desvenlafaxine)?
Pristiq is the brand name for desvenlafaxine succinate, a serotonin-norepinephrine reuptake inhibitor (SNRI) manufactured as an extended-release tablet for once-daily oral dosing.
Pristiq’s FDA Approval Status and Off-Label Use for Anxiety
FDA approval and off-label status:
- Approved indication: Major depressive disorder (MDD) in adults: approved February 29, 2008 by the FDA under the brand name Pristiq.
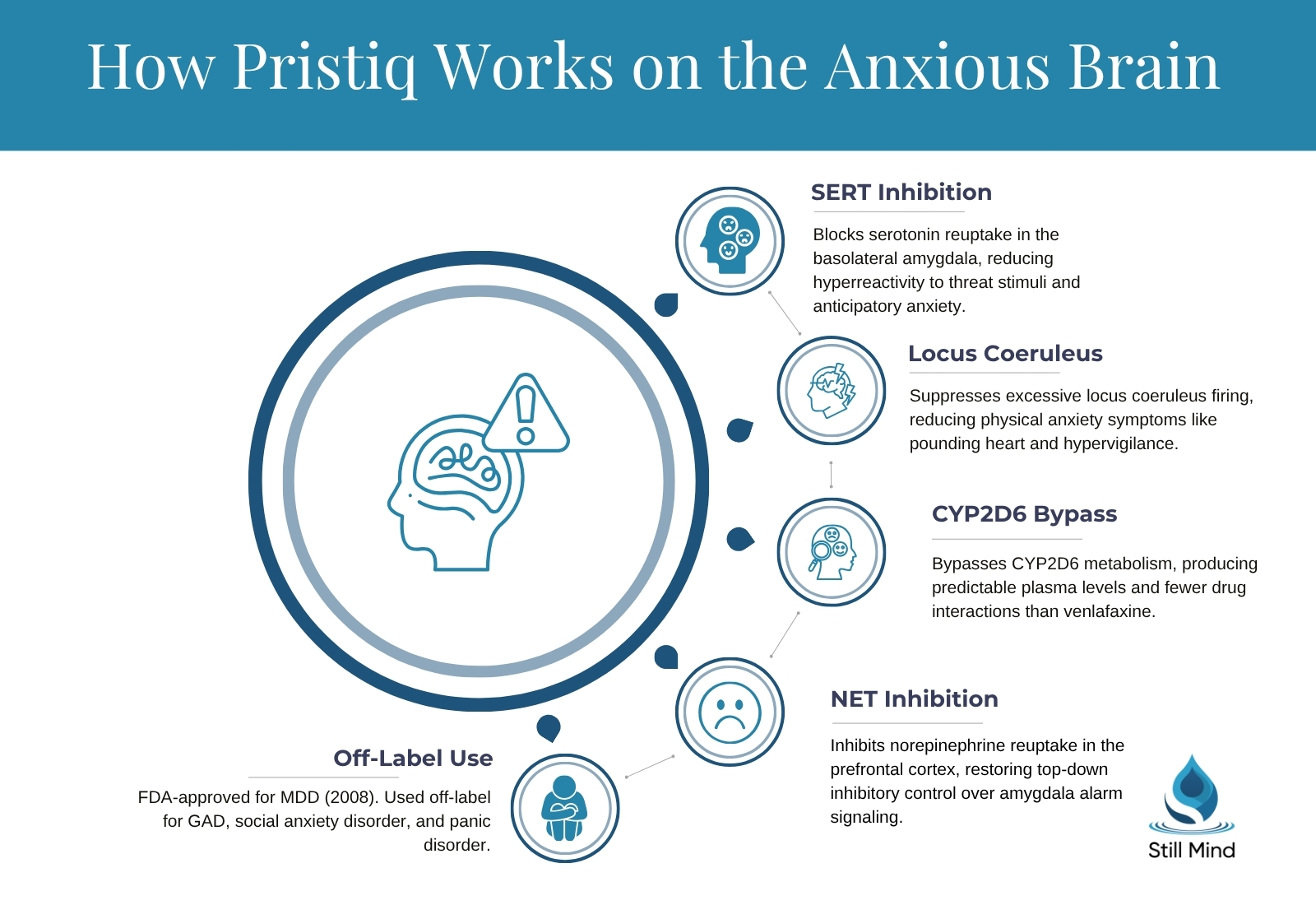
- Off-label indications: GAD, social anxiety disorder (SAD), panic disorder, and perimenopausal vasomotor symptoms with comorbid mood disruption.
- Not approved for: Pediatric or adolescent populations; Pristiq carries the same black box warning for increased suicidality in patients under 24 as other antidepressants.
- Clinical trial support: A completed Phase 4 randomized double-blind trial (NCT01316302) evaluated Pristiq 50–100 mg/day for generalized social anxiety disorder and found statistically significant reductions on the Liebowitz Social Anxiety Scale (LSAS) versus placebo.
How Pristiq Differs from Effexor (Venlafaxine)
Desvenlafaxine is the major active metabolite of venlafaxine (Effexor XR), meaning it delivers the same pharmacologically active compound that most venlafaxine metabolizers produce in the body.
Key pharmacological differences:
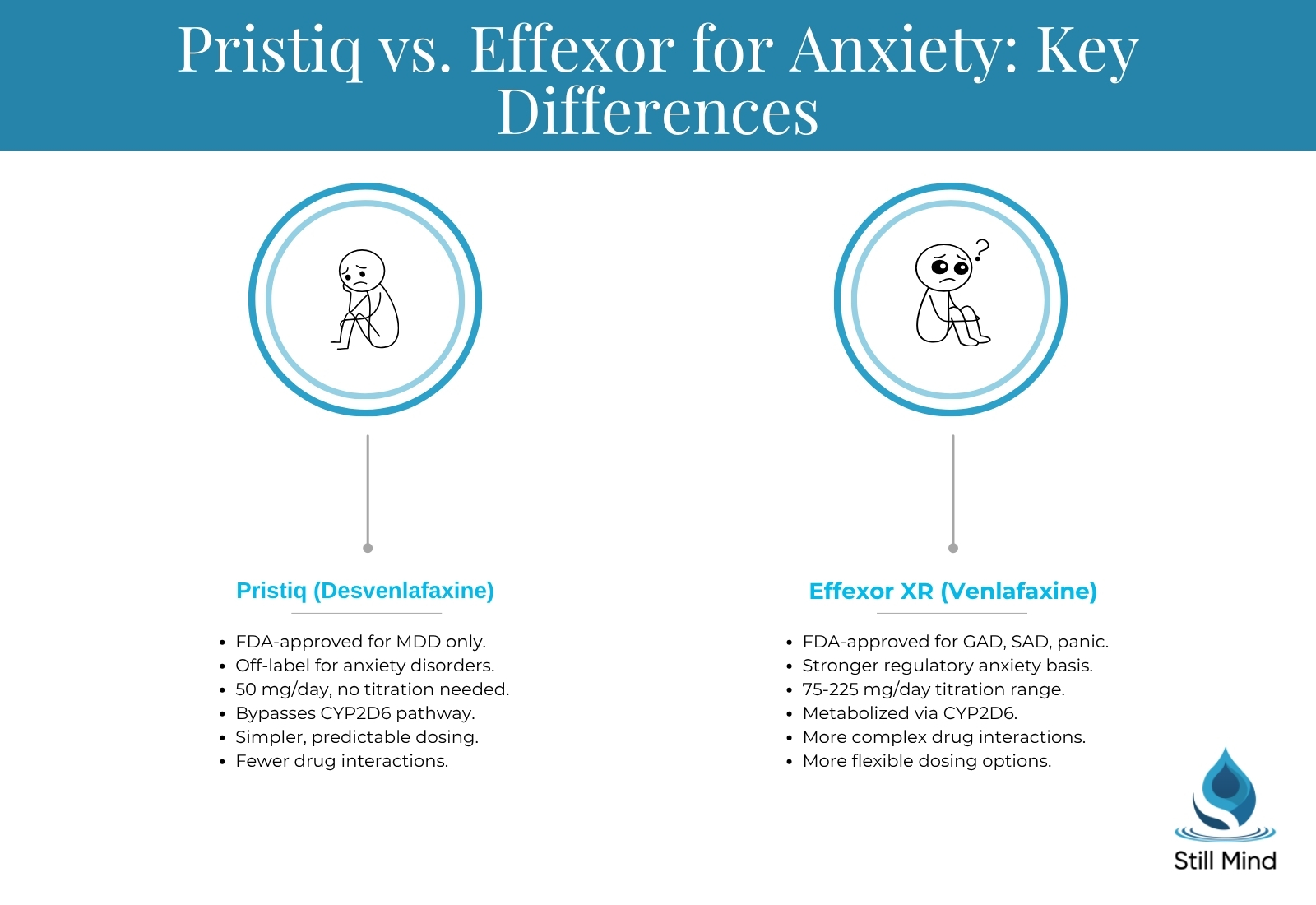
- Metabolic pathway: Desvenlafaxine does not require hepatic conversion through CYP2D6, which approximately 7–10% of the population metabolizes poorly; this makes Pristiq more pharmacokinetically predictable in those patients.
- Dosing simplicity: Pristiq has a single standard therapeutic dose of 50 mg/day; venlafaxine requires titration from 37.5 mg up to 75–375 mg/day depending on indication and response.
- Approved indications: Venlafaxine XR holds FDA approval for MDD, GAD, social anxiety disorder, and panic disorder: four indications versus Pristiq’s one. For anxiety specifically, venlafaxine carries stronger regulatory authorization.
- Bioavailability: Pristiq has approximately 80% absolute oral bioavailability with a Tmax of 7.5 hours, providing stable plasma levels throughout a 24-hour dosing interval.
Anxiety Disorders Pristiq Treats Off-Label
Psychiatrists prescribe desvenlafaxine across three primary anxiety presentations.
Off-label anxiety applications:
- Generalized anxiety disorder: Persistent, excessive worry across multiple life domains accompanied by somatic symptoms: muscle tension, fatigue, and sleep disruption: that norepinephrine upregulation from Pristiq can specifically address.
- Social anxiety disorder: Fear of negative evaluation in social or performance situations; norepinephrine modulation reduces the heightened sympathetic arousal (blushing, trembling, racing heart) that characterizes social anxiety more than purely serotonergic SSRIs do in some patients.
- Panic disorder: Recurrent unexpected panic attacks with anticipatory anxiety; the locus coeruleus norepinephrine system, which Pristiq suppresses via NET inhibition, directly mediates the alarm response underlying panic. For more on distinguishing these episodes, see panic attacks versus anxiety attacks.
How Pristiq Works on the Anxious Brain
Desvenlafaxine reduces anxiety by simultaneously elevating synaptic serotonin and norepinephrine concentrations in regions that regulate fear, threat detection, and emotional reactivity.
Serotonin and Norepinephrine Reuptake Inhibition in Anxiety Circuits
Neurobiological mechanisms:
- SERT inhibition in the amygdala: Desvenlafaxine occupies the serotonin transporter (SERT) in the basolateral amygdala, reducing amygdala hyperreactivity to threat stimuli: the core neurobiological substrate of worry and anticipatory anxiety.
- NET inhibition in the prefrontal cortex: Norepinephrine transporter (NET) blockade increases norepinephrine availability in the prefrontal cortex, restoring top-down inhibitory control over the amygdala’s alarm signaling.
- Locus coeruleus modulation: Desvenlafaxine suppresses excessive firing of the locus coeruleus, the brainstem nucleus that generates the norepinephrine-driven physical symptoms of anxiety: pounding heart, hypervigilance, and startle response.
- SERT/NET selectivity ratio: Pristiq has a higher affinity for SERT than NET (ratio approximately 10:1), producing its anxiolytic and antidepressant effects primarily through serotonin upregulation with meaningful norepinephrine augmentation at therapeutic doses.
The CYP2D6 Pathway and Drug Interaction Advantage
Because desvenlafaxine does not rely on CYP2D6 for activation, patients who are poor CYP2D6 metabolizers receive the same drug exposure as extensive metabolizers, eliminating a common source of SNRI treatment failure.
Clinical implications of CYP2D6 bypass:
- Reduced drug interactions: Medications that inhibit CYP2D6: including fluoxetine, paroxetine, bupropion, and many antipsychotics: elevate venlafaxine levels unpredictably; these interactions do not meaningfully affect Pristiq plasma levels.
- Predictable plasma levels: The extended-release formulation maintains steady-state plasma concentrations with minimal peak-to-trough variability, supporting consistent anxiolytic effect throughout the dosing cycle.
Why Some Patients Respond to Pristiq When SSRIs Fail
SSRIs target only the serotonin system, while SNRIs like Pristiq add norepinephrine modulation: a mechanism particularly relevant for anxiety subtypes driven by sympathetic hyperactivation rather than purely serotonergic dysregulation.
SNRI advantage in treatment-resistant anxiety:
- Somatic anxiety symptoms: Physical manifestations of anxiety: muscle tension, trembling, elevated heart rate, and sweating: respond more directly to norepinephrine modulation than to serotonin alone, making dual-action SNRIs preferable in patients whose anxiety is predominantly somatic.
- Comorbid depression: When anxiety co-occurs with major depressive disorder (MDD), an SNRI addresses both conditions simultaneously with a single agent, reducing polypharmacy burden.
- SSRI partial responders: Patients who achieve 30–40% anxiety reduction on SSRIs but remain significantly symptomatic may gain additional benefit from NET inhibition when switched to an SNRI or when an SNRI is added as augmentation.
How Long Does Pristiq Take to Work for Anxiety?
Desvenlafaxine requires weeks: not days: to produce meaningful anxiety reduction because its therapeutic effects depend on receptor-level adaptations rather than immediate neurotransmitter flooding.
Week 1–2: Initial Adjustment Phase
Early-phase effects:
- Transient symptom worsening: SERT inhibition initially increases synaptic serotonin before autoreceptor downregulation occurs; this can temporarily worsen anxiety, insomnia, or agitation in the first 7–14 days.
- Common early side effects: Nausea, headache, dizziness, and dry mouth peak during week one and diminish as receptor adaptation proceeds.
- No immediate anxiolytic effect: Unlike benzodiazepines, which produce immediate GABA-A receptor modulation, desvenlafaxine requires sustained transporter occupancy for neuroadaptive changes to accumulate.
Week 2–4: Emerging Anxiolytic Effects
Mid-phase response:
- Sleep normalization: As norepinephrine regulation stabilizes, hypervigilance and sleep-onset difficulty: hallmarks of anxiety: begin to diminish between days 10 and 21.
- Reduced somatic reactivity: Physical anxiety symptoms (racing heart, chest tightness, excessive sweating) decrease as the locus coeruleus response dampens with sustained NET inhibition.
- Partial mood improvement: Patients often notice less emotional reactivity and improved stress tolerance before full anxiety reduction is established.
Week 4–8: Full Therapeutic Response
Full response window:
- Established anxiolytic effect: The HAM-A (Hamilton Anxiety Rating Scale): developed by Dr. Max Hamilton in 1959, measuring both psychic anxiety (worry, tension) and somatic anxiety (cardiovascular, respiratory, and gastrointestinal symptoms) on a 0–56 scale: typically shows clinically significant reductions (≥50% score decrease) by week 6–8.
- Cognitive improvement: Working memory, concentration, and the ability to disengage from worry-focused thought patterns improve as prefrontal cortex function normalizes under stable norepinephrine signaling.
- Evaluating non-response: Psychiatrists typically reassess the treatment plan if no clinically meaningful HAM-A improvement has occurred by week 8 at a therapeutic dose, considering dose adjustment, augmentation, or a medication switch. For patients with persistent symptoms, structured antidepressant therapy alongside psychotherapy typically produces better outcomes than medication alone.
Pristiq Side Effects and Who Should Avoid It
Desvenlafaxine carries a well-characterized side effect profile that overlaps with other SNRIs, with some adverse effects requiring proactive monitoring and dose adjustment.
Common Side Effects
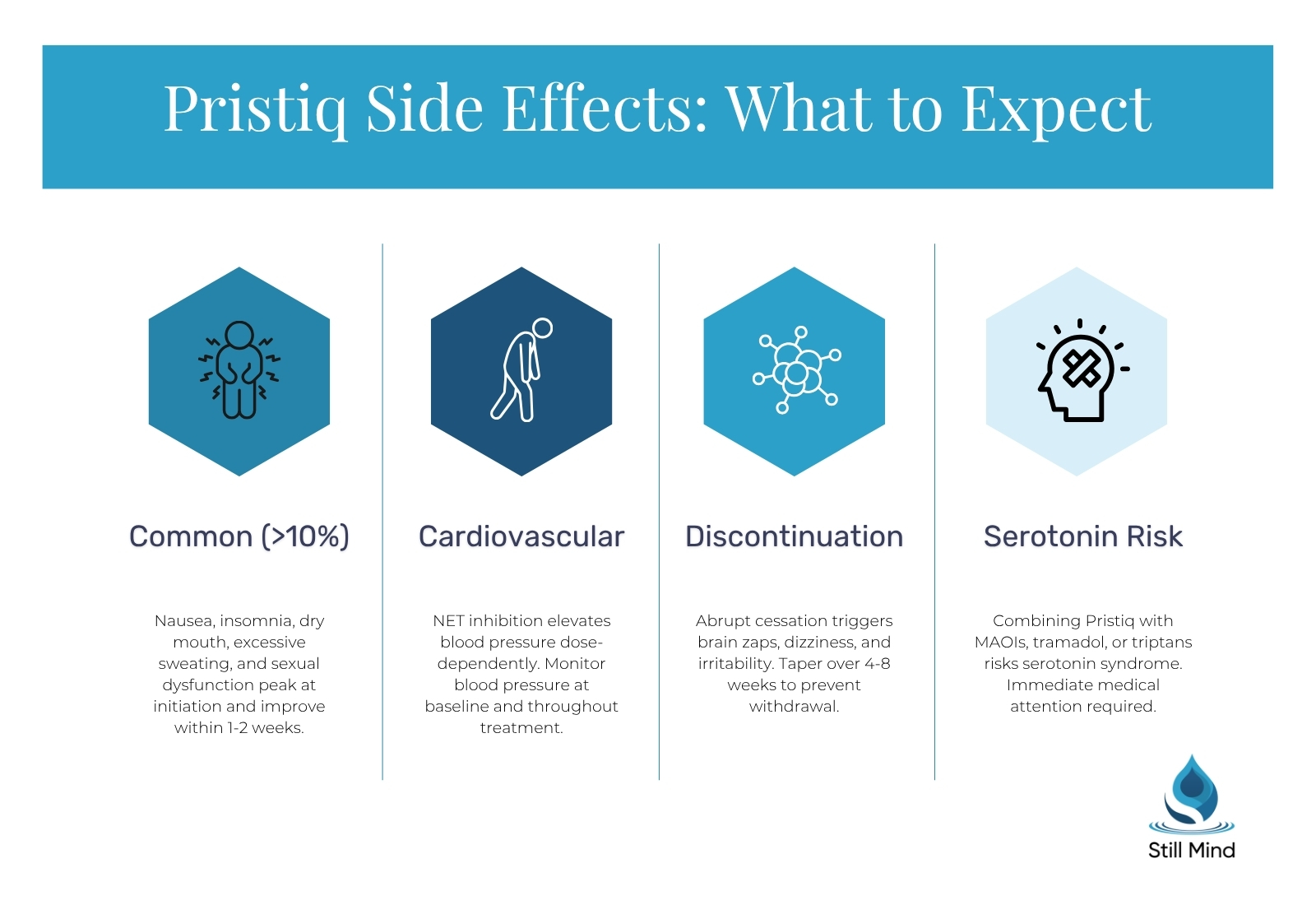
Frequently reported effects (occurring in >10% of patients):
- Nausea: Most common during dose initiation and typically resolves within 1–2 weeks; taking Pristiq with food reduces severity.
- Insomnia and sleep disruption: Elevated norepinephrine activity during the adjustment phase delays sleep onset; taking the dose in the morning rather than evening reduces this effect.
- Dry mouth: Anticholinergic-adjacent effect from norepinephrine upregulation; manageable with increased water intake.
- Excessive sweating: NET inhibition elevates noradrenergic tone in sweat gland innervation, producing hyperhidrosis in 10–14% of patients.
- Sexual dysfunction: Reduced libido, delayed orgasm, and anorgasmia affect approximately 20–30% of patients; the 2019 European Medicines Agency update added persistent sexual dysfunction as a labeled risk that may continue after discontinuation.
Severe and Serious Adverse Effects
Clinically significant adverse effects requiring monitoring:
- Elevated blood pressure: Norepinephrine reuptake inhibition produces dose-dependent blood pressure increases; baseline blood pressure should be measured before prescribing and monitored regularly, particularly at doses above 50 mg.
- Serotonin syndrome: Concurrent use of desvenlafaxine with MAOIs, triptans, tramadol, lithium, or other serotonergic agents elevates serotonin to potentially dangerous levels, producing agitation, hyperthermia, tachycardia, and myoclonus: a medical emergency requiring immediate intervention.
- Hyponatremia: SERT inhibition can cause syndrome of inappropriate antidiuretic hormone secretion (SIADH), producing dangerously low sodium levels particularly in elderly patients on diuretics.
- Increased bleeding risk: Desvenlafaxine reduces platelet serotonin stores, impairing platelet aggregation; patients on warfarin, NSAIDs, or aspirin require monitoring.
Long-Term Risks and Discontinuation Syndrome
Long-term considerations:
- Discontinuation syndrome: Abrupt cessation of desvenlafaxine triggers serotoninergic discontinuation syndrome within 24–72 hours, producing dizziness, “brain zaps” (brief electrical sensations), nausea, irritability, and insomnia; tapering over 4–8 weeks prevents most effects.
- Persistent sexual dysfunction: Post-SSRI/SNRI sexual dysfunction (PSSD) has been reported in a subset of patients who remain sexually symptomatic after completing treatment; its prevalence is not fully established but prompted the 2024 Australia TGA label update.
- Weight changes: Weight gain is less common with Pristiq than with paroxetine or mirtazapine but can occur with long-term use.
Pristiq vs. Other Anxiety Medications
When prescribers weigh desvenlafaxine against alternatives, the comparison turns on FDA approval status, mechanism, side effect tolerability, and drug interaction potential.
| Medication | Class | FDA-Approved for Anxiety | Standard Dose (Anxiety) | Key Advantage for Anxiety | Key Limitation |
|---|---|---|---|---|---|
| Pristiq (desvenlafaxine) | SNRI | No (off-label) | 50 mg/day | Simple dosing; minimal CYP2D6 interaction | No FDA anxiety indication; lacks flexibility |
| Effexor XR (venlafaxine) | SNRI | Yes (GAD, SAD, panic) | 75–225 mg/day | Multiple FDA anxiety approvals; flexible dosing | CYP2D6 interactions; discontinuation severity |
| Lexapro (escitalopram) | SSRI | Yes (GAD) | 10–20 mg/day | Best tolerated SSRI; minimal drug interactions | No norepinephrine action; may miss somatic anxiety |
| Zoloft (sertraline) | SSRI | Yes (panic, PTSD, OCD, SAD) | 50–200 mg/day | Broad anxiety indications; extensive safety data | CYP2D6 inhibition at higher doses; GI side effects |
| Cymbalta (duloxetine) | SNRI | Yes (GAD) | 60–120 mg/day | FDA-approved for GAD; beneficial for pain comorbidity | Significant CYP2D6 inhibition; liver monitoring required |
Pristiq Dosage for Anxiety
Off-label Pristiq dosing for anxiety follows the same parameters as MDD dosing, with the standard 50 mg/day dose applying to most patients regardless of anxiety subtype.
Standard Starting Dose and Initiation Strategy
Dosing protocol:
- Standard therapeutic dose: 50 mg once daily, taken with or without food; this is simultaneously the starting dose and the target maintenance dose for most patients, as higher doses provide no proven additional anxiolytic benefit.
- Sensitive patient initiation: Psychiatrists sometimes start at 25 mg/day for one to two weeks in patients with anxiety sensitivity to medication side effects, then increase to 50 mg; the 25 mg tablet is available for this purpose.
- Timing: Morning dosing is preferred when insomnia is a concern; the extended-release formulation sustains plasma levels across the full 24-hour dosing interval regardless of meal timing.
When Dosage Adjustments Are Made
Adjustment scenarios:
- Partial responders at 50 mg: Some prescribers increase to 100 mg/day after 4–6 weeks if anxiety reduction is partial; clinical evidence for improved efficacy at 100 mg versus 50 mg for anxiety specifically is limited.
- Renal impairment: Severe renal impairment (creatinine clearance <30 mL/min) requires dose reduction to 25–50 mg/day; desvenlafaxine is primarily renally cleared, unlike many other SNRIs that rely more on hepatic metabolism.
- Elderly patients: No dose adjustment is required by age alone, but blood pressure monitoring is especially important in older adults due to the noradrenergic cardiovascular effects of NET inhibition.
Maximum Dose and High-Dose Considerations
Upper dosing range:
- Maximum approved dose: 100 mg/day for MDD; doses above this have been studied (up to 400 mg/day) but demonstrate diminishing antidepressant returns with meaningfully increased side effects, particularly hypertension and tachycardia.
- Clinical consensus: Most prescribers and the 2024 Psychopharmacology Institute guidelines recommend 50 mg/day as the optimal dose for the majority of patients, reserving 100 mg for documented partial responders after an adequate trial at the lower dose.
Treatment for Anxiety at Still Mind
Still Mind provides integrated anxiety treatment that combines psychiatric medication management with evidence-based psychotherapies, recognizing that antidepressant therapy alone produces suboptimal outcomes compared to combined treatment approaches.
Psychiatric Evaluation and Medication Management
Medication management approach:
- Comprehensive psychiatric assessment: Prescribers at Still Mind evaluate anxiety subtype, severity (using validated scales including the HAM-A and GAD-7), comorbid conditions, and prior medication history before selecting a pharmacological approach.
- Medication selection: Desvenlafaxine and other SNRIs are considered alongside SSRIs, buspirone, and other options based on the patient’s specific anxiety presentation, medical history, and drug interaction profile.
- Integrated monitoring: Blood pressure, sleep quality, and treatment response are tracked systematically throughout the medication trial period. [CLIENT INPUT NEEDED: Specific monitoring frequency and psychiatric staffing ratios at Still Mind.]
Cognitive Behavioral Therapy for Anxiety
CBT components for anxiety:
- Cognitive restructuring: Cognitive behavioral therapy (CBT) targets the catastrophic appraisal patterns that maintain anxiety disorders: the core mechanism that pharmacotherapy alone cannot address.
- Exposure therapy: Systematic exposure to feared situations and somatic sensations reduces avoidance behaviors that perpetuate anxiety over time, working synergistically with the neurobiological changes that Pristiq produces.
- Combined treatment evidence: Meta-analyses consistently show that combined CBT and antidepressant treatment produces superior outcomes to either modality alone in GAD and social anxiety disorder, with lower relapse rates after medication discontinuation.
Dialectical Behavior Therapy Skills for Anxiety and Emotional Dysregulation
DBT skills application:
- Distress tolerance: Dialectical behavior therapy (DBT) distress tolerance skills: including the TIPP skill (Temperature, Intense Exercise, Paced Breathing, Progressive Relaxation): reduce acute anxiety activation without reliance on avoidance or reassurance-seeking.
- Emotion regulation: DBT emotion regulation modules directly target the emotional dysregulation that sustains anxiety disorders, building internal capacity that complements Pristiq’s neurobiological effects.
- Dual diagnosis integration: Patients whose anxiety co-occurs with substance use or other mental health conditions access dual diagnosis treatment that addresses both conditions concurrently rather than sequentially. [CLIENT INPUT NEEDED: Specific dual diagnosis program structure and eligibility criteria at Still Mind.]
Frequently Asked Questions
Will Pristiq calm anxiety?
Pristiq reduces anxiety symptoms by elevating serotonin and norepinephrine in anxiety-regulating brain regions, but it does not produce immediate calming: effects build over 2–8 weeks. For acute anxiety relief during the initiation period, prescribers sometimes add short-term buspirone or a low-dose benzodiazepine on a time-limited basis while desvenlafaxine reaches its full therapeutic level.
Is Lexapro or Pristiq better for anxiety?
Neither is universally superior. Lexapro (escitalopram) is FDA-approved for GAD and has an extensive tolerability record, making it the most common first-line choice. Pristiq is preferred when norepinephrine augmentation is needed: particularly when somatic anxiety symptoms dominate, when comorbid depression is present, or when CYP2D6 interactions complicate SSRI dosing. Prescribers individualize the choice based on prior medication history and specific anxiety presentation.
What is the best medication for anxiety and overthinking?
First-line evidence-based medications for anxiety and ruminative thinking include SSRIs (escitalopram, sertraline) and SNRIs (venlafaxine, desvenlafaxine). SSRIs are typically tried first; SNRIs are added or substituted when somatic anxiety is prominent or SSRI response is inadequate. Buspirone is a non-sedating alternative for GAD without the dependency risk of benzodiazepines. The optimal choice depends on the specific anxiety disorder, comorbidities, and individual response history.
What does taking Pristiq feel like?
During the first two weeks, many patients notice mild nausea, heightened activation, and occasionally worsened sleep. As the drug reaches steady state, patients typically describe reduced physical anxiety symptoms: less heart racing, less sweating, and improved stress tolerance: alongside mood stabilization. Unlike benzodiazepines, Pristiq produces no euphoria, no sedation, and no rapid relief; the experience is a gradual shift toward baseline rather than a noticeable pharmacological effect.
How long does Pristiq take to work for anxiety?
Initial improvements in sleep and somatic anxiety symptoms typically emerge at 2–4 weeks. Full anxiolytic response: meaningful reductions in worry, avoidance, and physical anxiety across daily life: generally requires 4–8 weeks at the therapeutic dose of 50 mg/day. If no clinically significant improvement has occurred by week 8, prescribers typically reassess dose, consider augmentation, or evaluate a medication switch.
Can Pristiq be used for panic disorder?
Pristiq is used off-label for panic disorder. Its norepinephrine reuptake inhibition targets the locus coeruleus firing patterns that drive the sympathetic surge underlying panic attacks, while serotonin upregulation reduces the anticipatory anxiety between attacks. Venlafaxine XR, Pristiq’s parent compound, holds FDA approval for panic disorder and serves as the better-established SNRI option; Pristiq is considered when venlafaxine is not tolerated or drug interactions make it unsuitable.
Is 25 mg of Pristiq effective for anxiety?
The 25 mg dose is primarily used as a brief initiation step to minimize early side effects in sensitive patients, not as a maintenance dose. Clinical trials establishing desvenlafaxine’s efficacy for anxiety used 50 mg/day; there is insufficient evidence that 25 mg produces meaningful anxiolytic benefit as a sustained therapeutic dose. Patients who find 50 mg intolerable should discuss alternative anxiolytic agents with their prescribers rather than remaining at a sub-therapeutic dose.
What can you add to Pristiq for anxiety?
Common augmentation strategies for partial Pristiq responders include buspirone (which enhances 5-HT1A receptor activity independently), low-dose atypical antipsychotics such as quetiapine or aripiprazole for treatment-resistant anxiety, and structured psychotherapy. Gabapentin is sometimes added for somatic anxiety or comorbid sleep disturbance. Benzodiazepines may be used short-term during initiation but are generally avoided as long-term co-treatments due to dependency risk and sedation. Any augmentation should be guided by a psychiatrist, not self-initiated.
References
- National Institute of Mental Health. (2024). Anxiety disorders: Epidemiology and prevalence data. https://www.nimh.nih.gov/health/statistics/any-anxiety-disorder
- U.S. Food and Drug Administration. (2008). Pristiq (desvenlafaxine) approval history and labeling. https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/021992s020lbl.pdf
- Psychopharmacology Institute. (2024). Desvenlafaxine guide: Pharmacology, indications, dosing guidelines and adverse effects. DOI: 10.64239/PI-BG005
- Hamilton, M. (1959). The assessment of anxiety states by rating. British Journal of Medical Psychology, 32(1), 50–55.
- Liebowitz, M. R., Tourian, K. A., Hwang, E., & Mendels, J. (2013). A double-blind, randomized study assessing the efficacy and tolerability of desvenlafaxine 10 and 50 mg/day over 8 weeks in adult outpatients with major depressive disorder. BMC Psychiatry, 13, 94.
- ClinicalTrials.gov. (Completed). NCT01316302: A 12-week double-blind, placebo-controlled, flexible-dose trial of Pristiq (desvenlafaxine) extended-release tablets in generalized social anxiety disorder.
- European Medicines Agency. (2019). PRAC recommendation: Persistent sexual dysfunction with SSRIs and SNRIs including desvenlafaxine. Pharmacovigilance Risk Assessment Committee.
- Substance Abuse and Mental Health Services Administration. (2023). Key substance use and mental health indicators in the United States: Results from the 2022 National Survey on Drug Use and Health. https://www.samhsa.gov/data/sites/default/files/reports/rpt39443/2022-nsduh-nnr.pdf
