




Schizoaffective disorder and schizophrenia are two distinct psychotic disorders, and the clinical difference between them determines the correct diagnosis, the right medications, and the most effective treatment path.
Both conditions involve hallucinations, delusions, and disorganized thinking. What separates schizoaffective disorder from schizophrenia is the presence of a significant mood episode, either a major depressive episode or a manic episode, that occurs alongside and independent of the psychotic symptoms.
That single distinction reshapes the entire treatment approach. In schizophrenia, antipsychotics alone form the pharmacological foundation. In schizoaffective disorder, mood-stabilizing agents or antidepressants must be added to address both symptom dimensions.
Understanding where these conditions overlap, and where they diverge, is what makes accurate diagnosis possible.
Key Takeaways
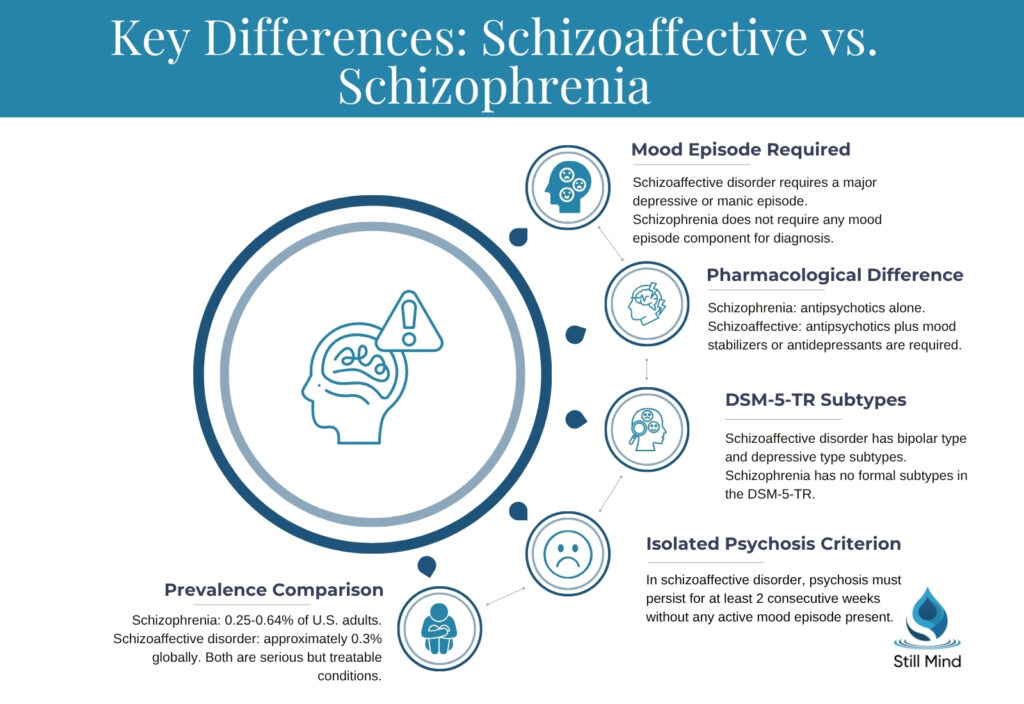
- Schizoaffective disorder requires a major depressive or manic episode to co-occur with active psychotic symptoms, a DSM-5-TR requirement that schizophrenia does not include.
- According to the National Institute of Mental Health, schizophrenia affects an estimated 0.25% to 0.64% of U.S. adults, while DSM-5-TR prevalence data estimates schizoaffective disorder affects approximately 0.3% of the general population.
- The DSM-5-TR classifies schizoaffective disorder into two subtypes: the bipolar type, which requires at least one manic episode, and the depressive type, which involves only major depressive episodes.
- Both conditions are chronic but treatable, and early, accurate diagnosis significantly improves long-term functional outcomes and reduces the risk of repeated psychiatric hospitalization.
What Are Schizoaffective Disorder and Schizophrenia?
Schizoaffective disorder and schizophrenia are both classified under schizophrenia spectrum and other psychotic disorders in the DSM-5-TR, sharing core features of reality distortion while differing in the presence and duration of mood episodes.
Schizophrenia: Definition and Core Criteria
The diagnostic criteria for schizophrenia require at least two of five symptom domains to be present for a minimum of six months, with at least one month of continuous active-phase symptoms.
DSM-5-TR diagnostic criteria for schizophrenia include at least two of the following:
- Hallucinations: Perceptual experiences without external stimulus, most commonly auditory hallucinations involving voices commenting on or conversing about the individual.
- Delusions: Fixed false beliefs resistant to rational correction, including persecutory, grandiose, and referential delusion types.
- Disorganized speech: Loosening of associations, tangential responses, or incoherence that disrupts meaningful communication.
- Grossly disorganized or catatonic behavior: Unpredictable agitation, waxy flexibility, or markedly reduced psychomotor activity that impairs daily functioning.
- Negative symptoms: Avolition, alogia, anhedonia, blunted affect, and asociality, each representing a reduction from the individual’s prior level of functioning.
Schizoaffective Disorder: Definition and Core Criteria
Schizoaffective disorder is defined in the DSM-5-TR as a condition in which a major mood episode, either depressive or manic, co-occurs with the active-phase psychotic symptoms of schizophrenia for a substantial portion of the illness duration.
DSM-5-TR criteria for schizoaffective disorder require all three of the following:
- Concurrent psychotic and mood symptoms: The full criteria for a major depressive or manic episode are met simultaneously with the active-phase criteria for schizophrenia.
- Isolated psychosis criterion: Hallucinations or delusions must persist for at least two consecutive weeks in the absence of a mood episode at some point during the total illness course.
- Mood episode predominance: A major depressive or manic episode must be present for the majority of the total active and residual illness duration, distinguishing schizoaffective disorder from schizophrenia with incidental mood disturbances.
How Each Condition Affects Brain Function
Both conditions involve disrupted dopaminergic neurotransmission, but schizoaffective disorder additionally involves the serotonergic and noradrenergic circuit dysregulation that drives sustained mood episodes.
Neurobiological Mechanisms in Schizophrenia
Schizophrenia involves hyperactivity of the mesolimbic dopamine pathway, which generates positive symptoms, combined with hypoactivity in the mesocortical pathway, which produces negative symptoms and cognitive impairment.
Core neurobiological features of schizophrenia include:
- Mesolimbic dopamine hyperactivity: Excess dopaminergic transmission in the mesolimbic pathway creates aberrant salience, assigning emotional significance to neutral stimuli and driving the hallucinations and delusional beliefs that define positive symptoms.
- Mesocortical dopamine deficit: Reduced prefrontal dopaminergic tone impairs working memory, executive function, and emotional expression, producing the avolition, blunted affect, and alogia that characterize the negative symptom cluster.
- NMDA receptor hypofunction: Glutamate NMDA receptor dysregulation in GABAergic interneurons disrupts cortical inhibitory control, amplifying both positive symptom severity and cognitive decline.
- Anosognosia: Impaired insight into one’s own illness, driven by prefrontal hypometabolism, affects the majority of people with schizophrenia and directly reduces treatment adherence and engagement with outpatient care.
Neurobiological Mechanisms in Schizoaffective Disorder
Schizoaffective disorder involves cross-diagnostic dopaminergic pathway disruption shared with schizophrenia, layered with the serotonin and norepinephrine dysregulation that underlies major depressive and manic episodes.
Neurobiological features distinguishing schizoaffective disorder:
- Cross-diagnostic dopaminergic pathway disruption: Disruption of dopamine circuits shared between psychotic and mood disorder pathways simultaneously drives both the psychotic and affective symptom dimensions, explaining the diagnostic complexity of schizoaffective disorder.
- Serotonin dysregulation in depressive type: Reduced serotonergic transmission in the limbic system drives persistent anhedonia, anergia, and hopelessness that co-occur with active psychosis in the depressive type.
- Mood-congruent psychotic features: Delusion content in schizoaffective disorder frequently reflects the dominant mood state, producing grandiose delusions during manic episodes and nihilistic delusions during major depressive episodes.
- Prefrontal-limbic dysconnectivity: Disrupted connectivity between the prefrontal cortex and the amygdala impairs emotional regulation and worsens with untreated mood cycling, a feature that distinguishes schizoaffective disorder from schizophrenia alone.
Schizoaffective Disorder vs. Schizophrenia: Key Differences
The presence and duration of mood episodes is the decisive clinical variable that separates schizoaffective disorder from schizophrenia, reshaping diagnostic criteria, medication requirements, and long-term prognosis.
| Feature | Schizophrenia | Schizoaffective Disorder |
|---|---|---|
| Primary symptom domain | Psychosis only | Psychosis plus sustained mood episodes |
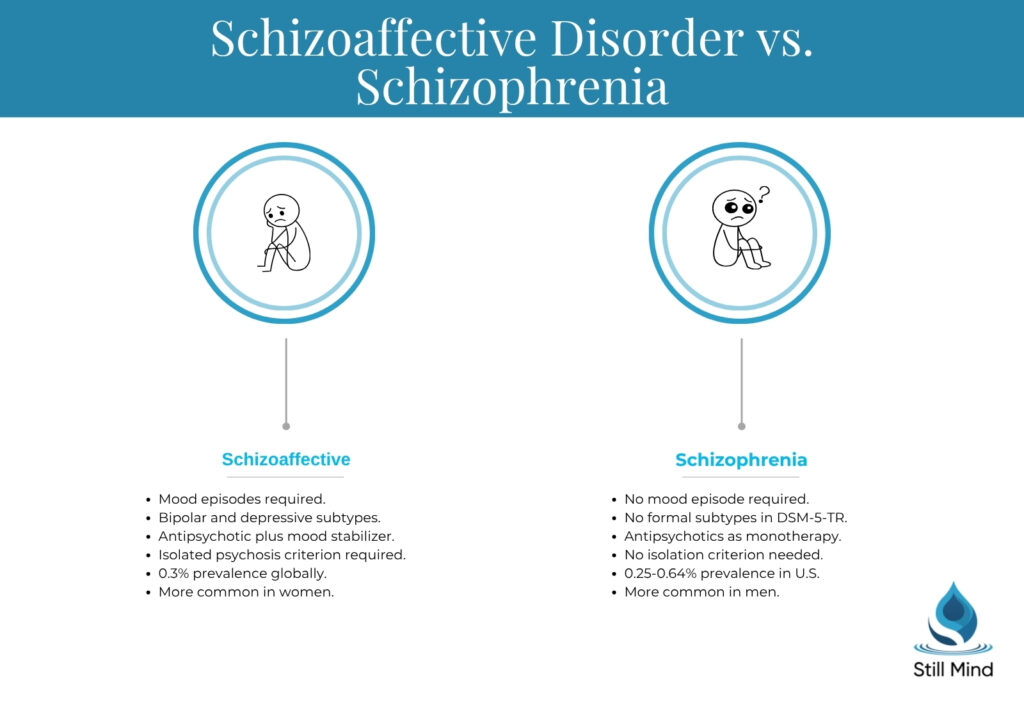
| Mood episode requirement | Not required | Required: major depressive or manic episode |
| Isolated psychosis criterion | Not applicable | Psychosis must persist at least 2 weeks without mood episode |
| Mood episode duration | Brief or absent | Must predominate throughout illness course |
| DSM-5-TR subtypes | None | Bipolar type and depressive type |
| First-line pharmacotherapy | Antipsychotics alone | Antipsychotics plus mood stabilizer or antidepressant |
| Estimated prevalence | 0.25%–0.64% of U.S. adults | Approximately 0.3% globally |
| More common in | Men | Women (particularly depressive type) |
| Prognosis without treatment | Progressive functional decline | Variable; worsened significantly by untreated mood cycling |
The bipolar type of schizoaffective disorder differs from primary bipolar disorder in that hallucinations and delusions persist independently of mood episodes, rather than occurring only during mood state peaks.
Symptoms of Schizoaffective Disorder and Schizophrenia
Overlapping psychotic symptoms make early differential diagnosis difficult without sustained longitudinal observation, which is why the Kraepelinian dichotomy of cleanly separated mood and psychotic disorders failed to account for conditions where both dimensions co-occur.
Symptoms of Schizophrenia
Schizophrenia produces positive, negative, and cognitive symptom dimensions, each reflecting distinct neurobiological disruptions in the mesolimbic and mesocortical dopamine pathways.
Positive symptoms of schizophrenia:
- Auditory hallucinations: Hearing voices that comment on the individual’s actions, issue commands, or converse with one another is the most diagnostically significant positive symptom and is present in the majority of schizophrenia cases.
- Persecutory delusions: Fixed, unshakeable beliefs that others intend harm, are monitoring the individual, or are conspiring against them represent the most common delusional subtype across the schizophrenia spectrum.
- Disorganized thought patterns: Tangential or incoherent speech, where ideas shift rapidly between unrelated topics, reflects the disrupted associative networks underlying formal thought disorder.
Negative symptoms of schizophrenia:
- Blunted affect vs. flat affect: Blunted affect refers to a reduced range of emotional expression, while flat affect refers to the near-complete absence of expressive response; both reflect mesocortical dopamine deficit rather than emotional absence.
- Avolition and alogia: Persistent inability to initiate goal-directed activity and poverty of verbal output reduce functional capacity independently of positive symptom severity and are frequently treatment-resistant.
Symptoms of Schizoaffective Disorder
Schizoaffective disorder produces the same positive and negative symptom profile as schizophrenia, with the addition of mood episode symptom criteria that must independently meet DSM-5-TR thresholds.
Mood symptoms specific to schizoaffective disorder:
- Depressive type symptoms: Persistent low mood or anhedonia lasting at least two weeks, accompanied by sleep disturbance, fatigue, and feelings of worthlessness, can converge with a psychotic break that intensifies during the depressive nadir.
- Bipolar type manic symptoms: Elevated or irritable mood, decreased need for sleep, pressured speech, grandiose delusions, and impulsive behavior co-occurring with active psychotic symptoms for at least one week define the bipolar type presentation.
- Independent psychotic symptoms: Between mood episodes, hallucinations and delusions persist for at least two consecutive weeks without any mood episode present, meeting the DSM-5-TR isolation criterion that distinguishes this condition from schizophrenia.
Shared Symptoms of Both Conditions
Both conditions share a psychotic symptom core that makes differential diagnosis impossible without assessing mood episode history, duration, and independence from active psychotic phases.
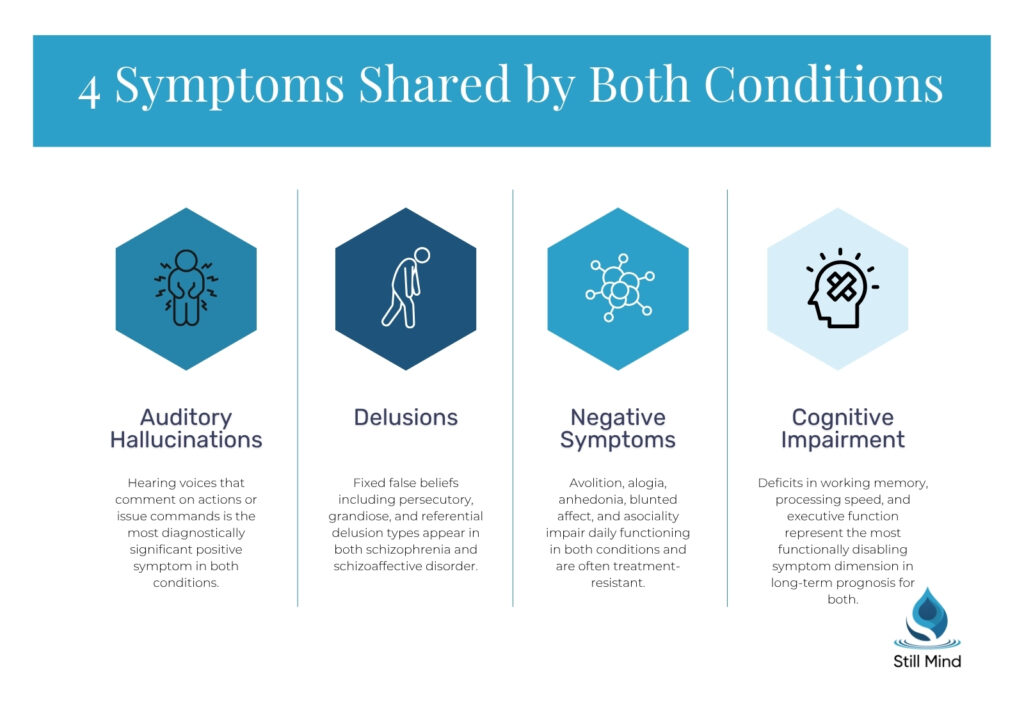
Symptoms common to both schizophrenia and schizoaffective disorder:
- Auditory and visual hallucinations: Both conditions produce sensory perceptions without external stimulus, with auditory hallucinations being the most prevalent form and the most diagnostically significant in each diagnosis.
- Negative symptom cluster: Social withdrawal, anhedonia, avolition, and blunted affect appear in both conditions and frequently persist even after positive symptoms are controlled with antipsychotic medication.
- Cognitive impairment: Deficits in working memory, processing speed, and executive function are present in both schizophrenia and schizoaffective disorder and represent the most functionally disabling symptom dimension in long-term prognosis.
Treatment for Schizoaffective Disorder and Schizophrenia
Effective treatment for both conditions requires a long-term combination of antipsychotic medication, structured psychotherapy, and psychosocial rehabilitation, with schizoaffective disorder additionally requiring pharmacological management of the mood dimension.
Medication Approaches
The pharmacological foundation for schizophrenia relies on antipsychotic monotherapy, while schizoaffective disorder requires a multi-agent regimen addressing both psychotic and affective symptom domains.
Medications for schizophrenia:
- Second-generation antipsychotics: Risperidone, olanzapine, quetiapine, and aripiprazole reduce positive symptoms by blocking D2 dopamine receptors in the mesolimbic pathway while minimizing the extrapyramidal effects associated with first-generation agents.
- Clozapine for treatment-resistant cases: For individuals who do not respond to two adequate antipsychotic trials, clozapine remains the only evidence-based pharmacological option, requiring regular hematological monitoring due to agranulocytosis risk.
Additional medications required for schizoaffective disorder:
- Mood stabilizers for bipolar type: Lithium and valproate augment antipsychotic therapy in bipolar type schizoaffective disorder, reducing manic episode frequency, severity, and the psychotic exacerbation that accompanies mood cycling.
- Antidepressants for depressive type: SSRIs and SNRIs are added to antipsychotic therapy in depressive type schizoaffective disorder to address the persistent major depressive episode dimension, though introduction requires caution to avoid precipitating manic episodes.
Psychotherapy and Behavioral Interventions
Evidence-based psychotherapy significantly improves functional outcomes in both conditions by building cognitive flexibility, relapse recognition skills, and emotional regulation capacity.
Evidence-based psychotherapy approaches:
- CBT for psychosis (CBTp): Cognitive behavioral therapy adapted for psychotic symptoms helps individuals evaluate delusional beliefs, reduce hallucination-related distress, and develop behavioral strategies that improve daily functioning alongside antipsychotic medication.
- Dialectical behavior therapy: Dialectical behavior therapy targets emotional dysregulation in schizoaffective disorder, building distress tolerance and interpersonal effectiveness skills that reduce mood episode severity.
- Supported employment and social skills training: Vocational rehabilitation and structured social interaction programs directly address the functional impairment driven by negative symptoms, improving community integration and long-term quality of life in both conditions.
Mental Health Treatment at Still Mind Florida
Still Mind Florida provides individualized outpatient mental health treatment for adults navigating schizophrenia spectrum disorders, schizoaffective disorder, and co-occurring mood and psychotic conditions.
Psychoeducation for Schizophrenia Spectrum Disorders
Psychoeducation at Still Mind Florida includes:
- Structured group and individual sessions that build symptom recognition, relapse prevention strategies, and medication adherence skills specific to schizophrenia spectrum and schizoaffective disorder presentations.
- Family-focused psychoeducation that equips caregivers with the clinical knowledge to recognize early decompensation warning signs and support consistent outpatient treatment engagement.
Holistic Mental Health Support
Holistic therapy at Still Mind Florida includes:
- Mind-body interventions integrated alongside evidence-based clinical care, supporting emotional regulation and stress reduction for individuals managing the sustained demands of schizoaffective disorder and schizophrenia.
- Individualized wellness programming addressing sleep, physical activity, and nutrition, each of which directly affects antipsychotic medication efficacy and mood episode stability in both conditions.
Clinical Assessment and Admissions
Getting started at Still Mind Florida:
- A comprehensive clinical intake assessment determines the appropriate level of outpatient care, identifies co-occurring conditions, and develops an individualized treatment plan aligned with DSM-5-TR diagnostic criteria for schizophrenia spectrum disorders.
- Clinical assessments are available to individuals seeking evaluation and support for acute schizophrenia spectrum or schizoaffective disorder presentations.
Frequently Asked Questions
What is the main difference between schizophrenia and schizoaffective disorder?
The main difference is the mood episode requirement. Schizophrenia involves hallucinations, delusions, and disorganized thinking without a required mood episode component. Schizoaffective disorder requires a major depressive or manic episode to co-occur with active psychosis, and those mood symptoms must predominate for the majority of the total illness duration.
Can people with schizoaffective disorder live alone?
Many people with schizoaffective disorder live independently with appropriate clinical support. Functional capacity depends on symptom severity, medication adherence, and access to consistent outpatient care. Individuals who maintain antipsychotic and mood-stabilizing regimens and engage in regular psychotherapy often achieve stable independent living with meaningful quality of life.
What are three signs of schizoaffective disorder?
Three core signs of schizoaffective disorder are hallucinations or delusions that persist independently of mood episodes, a major depressive or manic episode co-occurring with active psychotic symptoms, and sustained disruption of functioning across work, relationships, and self-care throughout both the psychotic and mood phases of the illness.
Can you recover from schizoaffective disorder?
Significant functional recovery is achievable for many individuals, and full remission occurs in some cases. Long-term antipsychotic and mood-stabilizing therapy combined with structured psychotherapy reduces relapse frequency. According to the National Institute of Mental Health, outcomes are consistently better when treatment begins early and continues without interruption.
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). American Psychiatric Publishing.
- National Institute of Mental Health. (2024). Schizophrenia. U.S. Department of Health and Human Services. https://www.nimh.nih.gov/health/topics/schizophrenia
- National Institute of Mental Health. (2024). Schizoaffective disorder. U.S. Department of Health and Human Services. https://www.nimh.nih.gov/health/statistics/schizoaffective-disorder
- Substance Abuse and Mental Health Services Administration. (2023). Key substance use and mental health indicators in the United States. https://www.samhsa.gov/data/report/2023-nsduh-annual-national-report
- Mayo Clinic. (2024). Schizophrenia: Symptoms and causes. Mayo Foundation for Medical Education and Research.
- Mayo Clinic. (2024). Schizoaffective disorder. Mayo Foundation for Medical Education and Research.
- Patel, K. R., Cherian, J., Gohil, K., & Atkinson, D. (2014). Schizophrenia: Overview and treatment options. P&T: A Peer-Reviewed Journal for Formulary Management, 39(9), 638–645.