




A panic attack is an abrupt surge of intense fear or extreme discomfort that reaches peak intensity within minutes and produces overwhelming physical and psychological symptoms that many people mistake for a heart attack or medical emergency.
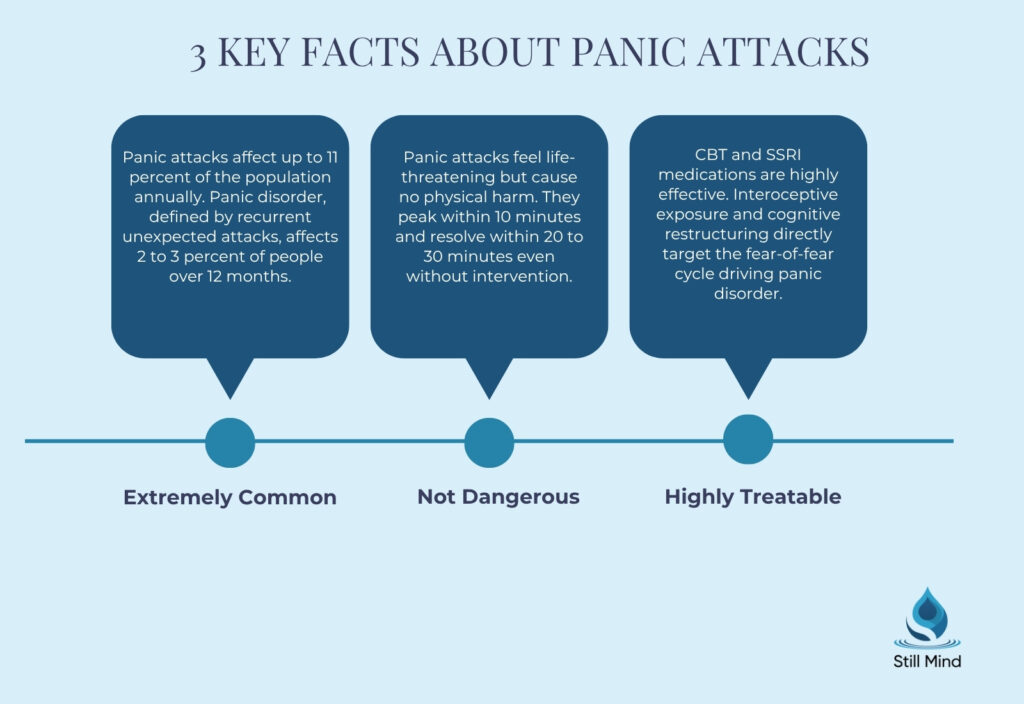
Panic attacks are not dangerous in themselves. But they feel life-threatening, and that experience alone shapes the avoidance behaviors, anticipatory anxiety, and functional impairment that follow repeated attacks.
Understanding what causes a panic attack, how to recognize one, and how to stop it are the three questions that matter most for anyone navigating this experience.
Key Takeaways
- According to the Merck Manual, panic attacks affect as much as 11 percent of the population in any given year, while panic disorder, the condition defined by recurrent unexpected panic attacks, affects 2 to 3 percent of the population over a 12-month period.
- The DSM-5-TR defines a panic attack as an abrupt surge of intense fear or discomfort reaching peak intensity within minutes, accompanied by at least 4 of 13 specific physical and cognitive symptoms.
- According to the National Institute of Mental Health, panic disorder typically begins in late adolescence or early adulthood and affects women approximately twice as often as men.
- Research from the NIH StatPearls database identifies amygdala dysregulation and chemical imbalances in GABA, cortisol, and serotonin as the primary neurobiological mechanisms underlying panic disorder.
What Is a Panic Attack?
A panic attack is a discrete episode of abrupt, intense autonomic nervous system activation that peaks within minutes, producing a cluster of physical and cognitive symptoms that mimic the physiological profile of genuine life-threatening danger.
DSM-5-TR Definition and Diagnostic Criteria
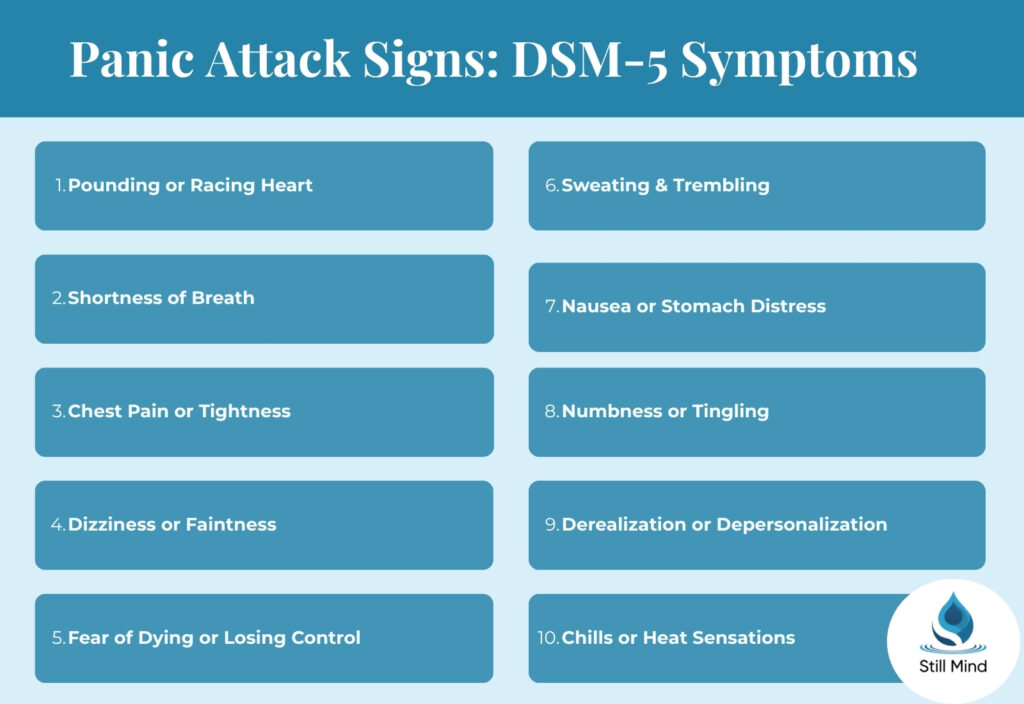
The DSM-5-TR defines a panic attack as an abrupt surge of intense fear or discomfort with a distinct peak within minutes, accompanied by four or more of the following thirteen symptoms.
DSM-5-TR panic attack symptoms:
- Cardiovascular symptoms: Palpitations, pounding heartbeat, or accelerated heart rate; chest pain or discomfort.
- Respiratory symptoms: Sensations of shortness of breath or smothering; feelings of choking.
- Neurological symptoms: Dizziness, unsteadiness, lightheadedness, or faintness; paresthesias including numbness or tingling sensations; chills or heat sensations.
- Gastrointestinal symptoms: Nausea or abdominal distress.
- Dissociative symptoms: Derealization, the feeling that surroundings are unreal; depersonalization, the feeling of being detached from oneself.
- Cognitive symptoms: Fear of losing control or “going crazy”; fear of dying.
- Other physical symptoms: Sweating; trembling or shaking.

Expected vs. Unexpected Panic Attacks
The DSM-5-TR distinguishes between two panic attack types based on the presence or absence of an identifiable situational trigger.
Clinical distinction:
- Unexpected panic attacks: Occur without any identifiable situational cue or trigger, arising spontaneously during ordinary activity or even during sleep. Recurrent unexpected panic attacks are the defining feature of panic disorder.
- Expected panic attacks: Occur reliably in response to a specific situational cue, such as heights, blood draws, or crowded spaces. These are more characteristic of specific phobias and social anxiety disorder than of panic disorder.
Why Panic Attacks Happen: Brain and Body
Panic attacks result from aberrant activation of the brain’s threat detection and emergency response systems, producing the physiological cascade of fight-or-flight activation in the complete absence of genuine external danger.
Amygdala Dysregulation and the Fear Circuit
The amygdala, the brain’s primary threat evaluation center, plays the central role in generating panic attacks by misfiring the alarm signal that initiates the autonomic nervous system’s emergency response.
The neurobiological mechanism:
- Amygdala hyperreactivity: In panic disorder, the amygdala generates an intense alarm response to internal sensory cues, such as mild heart rate elevation, that would not activate this system in individuals without the disorder. This misinterpretation of benign interoceptive signals as life-threatening triggers the full sympathetic nervous system cascade.
- Sympathoadrenal activation: The amygdala alarm signal activates the hypothalamic-pituitary-adrenal (HPA) axis, driving cortisol and adrenaline release that produces the cardiovascular, respiratory, and muscular symptoms experienced during a panic attack.
- Fear of fear cycle: The initial panic attack creates a conditioned fear of the physical sensations themselves, so that subsequent experiences of normal arousal, such as a racing heart during exercise, trigger anticipatory anxiety that amplifies into a full panic attack.
GABA, Serotonin, and Cortisol Dysregulation
Neurochemical contributors to panic attacks:
- GABA deficit: Gamma-aminobutyric acid (GABA), the brain’s primary inhibitory neurotransmitter, normally suppresses excessive sympathetic nervous system activation. Reduced GABAergic tone in panic disorder reduces the brain’s ability to dampen the alarm response, making panic attacks more likely to reach full intensity.
- Serotonin pathway dysregulation: Disrupted serotonergic transmission in the limbic system and prefrontal cortex impairs emotional regulation and threat appraisal accuracy, contributing to the hypervigilance for bodily sensations that precedes panic episodes.
- Cortisol hypersensitivity: Elevated baseline cortisol in individuals with panic disorder produces a state of chronic, low-level physiological arousal that lowers the threshold for full panic attack activation in response to minimal stressors.
What Causes a Panic Attack? Triggers by Category
Panic attacks arise from a range of physiological, psychological, environmental, and substance-related triggers, with some individuals experiencing no identifiable trigger at all.
Psychological and Emotional Triggers
Psychological causes of panic attacks:
- Chronic stress and emotional exhaustion: Sustained psychological stress elevates cortisol and reduces GABAergic inhibitory capacity, producing the neurochemical conditions that make panic attacks significantly more likely to occur.
- Trauma and PTSD: Post-traumatic stress disorder generates panic attacks through trauma-related hyperarousal, with sudden sensory reminders of the traumatic event activating the full sympathoadrenal cascade even in objectively safe environments.
- Generalized anxiety disorder: Chronic worry and hypervigilance maintain elevated sympathetic nervous system tone, reducing the threshold at which benign physical sensations are misappraised as dangerous and triggering the escalation to a full panic attack.
Medical and Physiological Triggers
Medical causes of panic attacks:
- Hyperthyroidism: Excess thyroid hormone directly elevates heart rate, body temperature, and metabolic rate, producing the palpitations, sweating, and trembling that are physiologically indistinguishable from panic attack symptoms and can directly precipitate panic episodes.
- Cardiac arrhythmias: Irregular heart rhythms produce palpitations and chest discomfort that trigger the catastrophic appraisal of cardiac danger, activating the fear circuit and escalating into a panic attack through the fear of fear mechanism.
- Hypoglycemia: Rapid blood glucose drops activate the sympathoadrenal response, producing sweating, shakiness, racing heart, and lightheadedness that can trigger panic attacks in susceptible individuals.
Substance and Medication Triggers
Substance-related causes of panic attacks:
- Caffeine and stimulants: High caffeine intake elevates sympathetic nervous system arousal and produces palpitations and jitteriness that individuals with panic disorder frequently misappraise as the onset of a panic attack, triggering the self-fulfilling escalation pattern.
- Cannabis: In susceptible individuals, cannabis produces tachycardia, depersonalization, and derealization that closely mimic panic attack symptoms and frequently precipitate full panic episodes, particularly in those with no prior cannabis tolerance.
- Benzodiazepine and alcohol withdrawal: Abrupt withdrawal from benzodiazepines or alcohol reduces GABAergic inhibitory capacity precipitously, producing the neurochemical conditions for intense, recurrent panic attacks as a core withdrawal symptom.
Genetic and Family History
Hereditary contributors:
- First-degree relative history: Individuals with a first-degree biological relative with panic disorder face a 40 percent increased risk of developing the condition, reflecting the heritable nature of amygdala reactivity, GABA function, and HPA axis sensitivity.
- Shared genetic architecture with depression: Panic disorder shares genetic risk factors with major depressive disorder, which explains the high rates of co-occurrence between the two conditions and the effectiveness of SSRIs in treating both.
Signs of a Panic Attack: How to Recognize One
Recognizing a panic attack as it occurs is clinically significant because accurate identification interrupts the catastrophic appraisal cycle that amplifies and prolongs the episode.
Physical Signs of a Panic Attack
Physical symptoms of a panic attack reflect full sympathoadrenal activation and emerge rapidly, reaching peak intensity within 10 minutes of onset.
Physical signs to recognize:
- Cardiovascular: Racing or pounding heart, chest tightness or pain, feeling of impending cardiac crisis.
- Respiratory: Difficulty breathing, sensation of not getting enough air, shortness of breath without exertion.
- Neurological: Dizziness, lightheadedness, tingling or numbness in hands, face, or feet, hot flashes or chills.
- Gastrointestinal: Nausea, stomach cramping, or urgent need to use the bathroom.
Psychological Signs of a Panic Attack
Psychological signs to recognize:
- Derealization and depersonalization: The world appearing suddenly unreal, dream-like, or distant, or the feeling of observing oneself from outside the body, are among the most disorienting psychological symptoms of a panic attack and frequently drive emergency room presentations.
- Fear of dying: The acute conviction that one is having a heart attack or is about to die reflects the brain’s misinterpretation of sympathoadrenal activation as a genuine medical emergency.
- Fear of losing control: The fear of fainting, losing behavioral control, or “going crazy” in a public setting drives the avoidance behaviors that develop following recurrent panic attacks.
Panic Attack vs. Heart Attack
Critical clinical distinction:
- Panic attack: Symptoms peak within 10 minutes, typically resolve within 20 to 30 minutes, are not associated with ST-segment ECG changes, and are produced by psychological rather than cardiac pathology.
- Heart attack: Chest pain is typically described as pressure, squeezing, or radiation to the jaw and left arm; does not resolve spontaneously; is associated with ECG changes and elevated cardiac enzymes. When uncertain, seek emergency medical evaluation immediately.
How to Calm Down During a Panic Attack
The most evidence-supported immediate interventions for panic attacks interrupt the physiological cascade by directly reducing sympathetic nervous system activation and correcting the cognitive misappraisal that sustains the episode.
Immediate Calming Techniques
Evidence-based calming strategies:
- Diaphragmatic breathing: Slow, controlled breathing activates the parasympathetic nervous system through the respiratory vagal reflex, directly counteracting sympathoadrenal activation. Inhale for 4 counts, hold for 1, exhale for 6 counts, repeating until heart rate decreases.
- Cognitive reappraisal: Consciously identifying the experience as a panic attack rather than a medical emergency interrupts the catastrophic appraisal cycle. The explicit acknowledgment that the symptoms are uncomfortable but not dangerous reduces the secondary fear layer that amplifies attack intensity.
- Grounding techniques: Sensory grounding methods such as the 5-4-3-2-1 technique, identifying five things you can see, four you can touch, three you can hear, two you can smell, and one you can taste, redirect attentional resources from internal bodily monitoring to external environmental anchors.
Long-Term Treatment to Prevent Panic Attacks
Evidence-based treatment approaches:
- Cognitive behavioral therapy: Cognitive behavioral therapy is the most evidence-supported long-term treatment for panic disorder, combining interoceptive exposure exercises that systematically desensitize individuals to feared bodily sensations with cognitive restructuring that corrects the catastrophic misappraisals that trigger panic.
- SSRIs and SNRIs: Selective serotonin reuptake inhibitors including sertraline, fluoxetine, and escitalopram are first-line pharmacological treatments for panic disorder, reducing both attack frequency and anticipatory anxiety through serotonergic pathway stabilization.
- Mindfulness-based interventions: Holistic and mindfulness-based approaches reduce the chronic sympathetic nervous system hyperarousal that lowers the panic attack threshold, building the sustained parasympathetic regulatory capacity that makes individual attacks less likely.
Mental Health Treatment at Still Mind Florida
Still Mind Florida provides outpatient mental health treatment for adults navigating panic disorder, anxiety disorders, trauma, and co-occurring mood conditions.
CBT-Based Anxiety Treatment
Outpatient anxiety care at Still Mind Florida:
- Structured CBT and interoceptive exposure programs aligned with DSM-5-TR diagnostic criteria for panic disorder, addressing both the acute attack cycle and the anticipatory anxiety and avoidance behaviors that develop following recurrent episodes.
- Individual and group therapy sessions building the cognitive reappraisal and nervous system regulation skills that reduce panic attack frequency and restore functional capacity in occupational and social domains.
Dialectical Behavior Therapy for Emotional Regulation
DBT skills for panic disorder:
- Dialectical behavior therapy distress tolerance skills directly address the panic attack experience by building the capacity to remain regulated through intense physiological arousal without engaging the catastrophic appraisal cycle that sustains and amplifies panic episodes.
- Clinical assessments for panic disorder and related anxiety conditions are available, with individualized treatment planning developed from comprehensive DSM-5-TR diagnostic evaluation.
Frequently Asked Questions
What are the main causes of panic attacks?
The main causes are amygdala hyperreactivity producing misfired fear responses, GABA and serotonin dysregulation reducing the brain’s inhibitory capacity, chronic stress and trauma history, genetic predisposition, and certain medical conditions including hyperthyroidism and cardiac arrhythmias. Substance use including high caffeine intake and cannabis can also directly trigger panic episodes.
How to calm down in a panic attack?
Use diaphragmatic breathing with a slow extended exhale to activate the parasympathetic nervous system. Remind yourself explicitly that this is a panic attack, not a medical emergency, to interrupt catastrophic appraisal. Use sensory grounding to redirect attention externally. Most panic attacks resolve within 20 to 30 minutes even without intervention.
How to recognize a panic attack?
A panic attack involves at least four simultaneous symptoms including racing heart, shortness of breath, dizziness, chest tightness, tingling sensations, sweating, nausea, derealization, or intense fear of dying or losing control, reaching peak intensity within 10 minutes. Unlike anxiety, which builds gradually, panic attacks arise abruptly and intensely with no warning.
How to avoid a panic attack?
Long-term avoidance requires treating the underlying panic disorder through CBT interoceptive exposure, SSRI pharmacotherapy, and lifestyle modifications including consistent sleep, reduced caffeine intake, regular aerobic exercise, and mindfulness practice. Avoidance of feared situations provides short-term relief but maintains and worsens panic disorder over time by preventing the habituation that reduces attack frequency.
References
- National Institute of Mental Health. (2024). Panic disorder. U.S. Department of Health and Human Services. https://www.nimh.nih.gov/health/topics/panic-disorder
- National Institutes of Health. (2023). Panic disorder. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK430973/
- Substance Abuse and Mental Health Services Administration. (2023). Key substance use and mental health indicators in the United States. https://www.samhsa.gov/data/report/2023-nsduh-annual-national-report
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). American Psychiatric Publishing.
- Merck Manual Professional. (2026). Panic attacks and panic disorder. Merck Manual.
- Cleveland Clinic. (2023). Panic attack and panic disorder. Cleveland Clinic Medical.
- Mayo Clinic. (2023). Panic attacks and panic disorder: Symptoms and causes. Mayo Foundation for Medical Education and Research.