




A BPD episode is an acute period of intense emotional dysregulation in borderline personality disorder (BPD). It is triggered by a perceived interpersonal threat and characterized by explosive rage, dissociation, suicidal urges, or a complete collapse of self-image, typically resolving within minutes to several hours.
A BPD episode is brief and reactive, emerging and subsiding faster than any other mood disorder but with an intensity that leaves individuals and those around them feeling exhausted, confused, and frightened. Understanding what triggers these episodes, what they look like from the outside, and which interventions actually work is the first step toward managing them.
Key Takeaways
- “BPD episode” is not a formal DSM-5-TR diagnostic term; it describes acute periods of emotional dysregulation that are a defining feature of borderline personality disorder, distinguishing it from mood episodes in bipolar disorder by their shorter duration and interpersonal trigger.
- According to NAMI, approximately 1.4% of the U.S. adult population meets diagnostic criteria for borderline personality disorder, with emotional dysregulation episodes representing the most common reason BPD patients seek emergency psychiatric care.
- Neurobiological research using fMRI shows that individuals with BPD have an amygdala that activates 2-3 times more intensely in response to neutral social stimuli compared to controls, and a prefrontal cortex that fails to adequately inhibit this activation.
- BPD episodes typically resolve within hours, not days: making duration the single most reliable clinical differentiator between BPD emotional instability and bipolar disorder mood episodes.
- Dialectical behavior therapy (DBT), developed specifically for BPD by Dr. Marsha Linehan, is the only treatment with robust evidence for reducing both the frequency and intensity of acute BPD episodes, particularly through its distress tolerance and emotion regulation skill modules.
What Is a BPD Episode?
A BPD episode is a period of acute emotional crisis that emerges rapidly in response to a perceived interpersonal threat and temporarily overwhelms the individual’s capacity to function or self-regulate.
“BPD Episode” Is Not a Formal Diagnosis: What the Term Actually Means
The DSM-5-TR does not use the term “episode” to describe Borderline Personality Disorder symptoms the way it does for mood disorders. The clinical concept closest to a “BPD episode” is Criterion 6 (affective instability due to a marked reactivity of mood) combined with the full constellation of nine BPD diagnostic criteria, including frantic efforts to avoid abandonment, unstable relationships, identity disturbance, and recurrent self-harm.
What the term describes in clinical and everyday use:
- Acute emotional decompensation: A rapid shift from relative stability to overwhelming emotional intensity in response to a specific trigger, most often an interpersonal event such as perceived rejection, criticism, abandonment, or invalidation.
- Temporary loss of emotional regulation: During an episode, individuals typically lose access to their reflective capacity and their ability to apply coping skills, experiencing emotions as all-consuming rather than manageable.
- Not equivalent to a psychotic episode or a mood episode: Unlike a bipolar manic or depressive episode lasting days to weeks, a BPD episode typically resolves within minutes to hours and does not involve the full neurobiological state shift of a primary mood disorder.
The Four Main Types of BPD Episodes
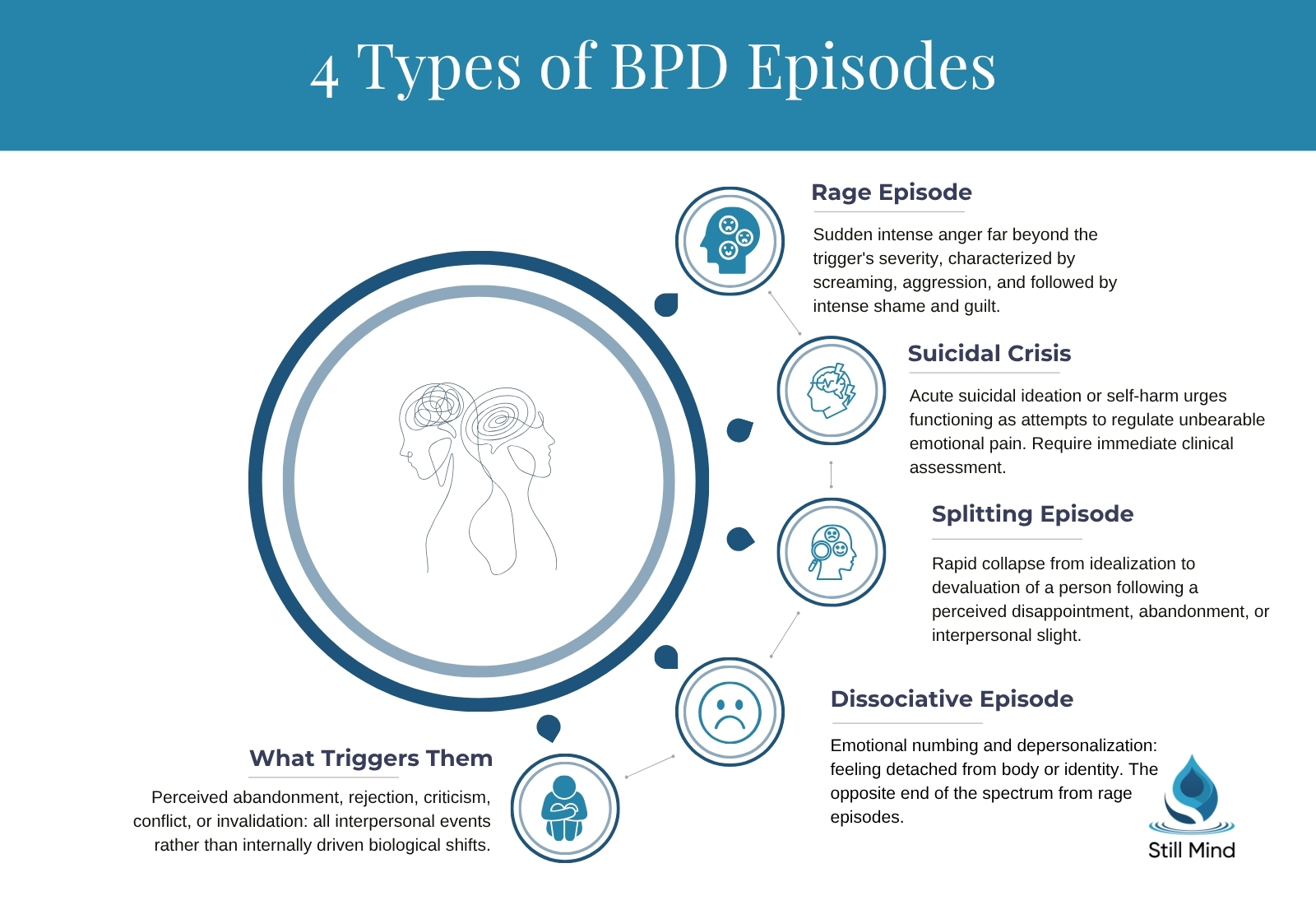
BPD episodes cluster into four primary presentations, each with distinct behavioral signatures and risk profiles.
Primary episode types:
- Rage and explosive episodes: Sudden, intense anger that escalates far beyond what the triggering situation would seem to warrant; characterized by screaming, throwing objects, verbal attacks, or physical aggression directed at self or others; often followed by intense shame and guilt.
- Dissociative episodes: Periods of emotional numbing, sometimes described as quiet BPD presentations, depersonalization (feeling detached from one’s body or identity), or derealization (the environment feeling unreal); these represent the opposite end of the emotional spectrum from rage episodes and may follow extreme stress or unmanageable emotional arousal.
- Suicidal crisis and self-harm episodes: Acute periods of suicidal ideation, self-harm urges, or self-harm behavior that function as attempts to regulate unbearable emotional pain, communicate distress, or punish the self; these require immediate clinical assessment and safety planning.
- Splitting-triggered episodes: Rapid collapse from idealization to devaluation of a person or relationship following a perceived disappointment or abandonment; characterized by all-or-nothing thinking that reorganizes the individual’s entire perception of a person from completely good to completely bad.
How the ZAN-BPD Scale Measures BPD Severity
The Zanarini Rating Scale for Borderline Personality Disorder (ZAN-BPD), developed by Dr. Mary Zanarini at McLean Hospital, measures the severity of the four affective, cognitive, impulsive, and interpersonal domains of BPD on a 0-36 scale, with higher scores indicating more severe symptom burden during the most recent week.
Clinicians use the ZAN-BPD to establish a baseline before treatment, track changes in episode frequency and intensity over time, and determine when a patient has achieved clinically significant improvement defined as a reduction in total score of at least 8 points. The scale captures both the subjective intensity of emotional dysregulation and the behavioral consequences of acute episodes, making it useful for identifying whether DBT or other interventions are producing measurable change.
What Causes and Triggers BPD Episodes
BPD episodes emerge from a specific combination of neurobiological vulnerability and interpersonal triggers that is distinct from the etiology of mood episodes in bipolar disorder.
Neurobiological Causes: Amygdala Hyperreactivity and Prefrontal Failure
The two-system neurobiological model:
- Amygdala hyperreactivity: Neuroimaging studies demonstrate that the amygdala in individuals with BPD produces exaggerated threat-detection responses to neutral or mildly emotional social stimuli, including neutral facial expressions that most people would not register as threatening; this hyperreactivity persists even after the triggering stimulus has been removed.
- Prefrontal cortex inhibitory failure: The dorsolateral prefrontal cortex (DLPFC) and the orbitofrontal cortex, which normally inhibit amygdala activation through top-down regulatory pathways, show reduced activity in BPD, allowing amygdala-driven emotional responses to proceed unchecked.
- Anterior cingulate cortex dysregulation: The ACC, which monitors emotional conflict and adjusts regulatory effort, shows abnormal connectivity patterns in BPD that further impair the integration of emotional information with rational appraisal during acute episodes.
Linehan’s Biosocial Model: Why BPD Episodes Are So Intense
Dr. Marsha Linehan, the psychologist who developed dialectical behavior therapy, proposed the biosocial model of BPD to explain how the disorder and its characteristic episodes develop: a biological predisposition to high emotional sensitivity (amplified amygdala reactivity and slow return to baseline) combines with an invalidating environment: caregivers who consistently dismiss, minimize, or punish the child’s emotional experiences: to produce the chronic emotional dysregulation that defines BPD.
Core elements of the biosocial model:
- Biological sensitivity: The individual experiences emotions more rapidly, more intensely, and with a slower return to baseline than neurotypical peers: what Linehan described as having emotional third-degree burns where others have intact skin.
- Invalidating environment: Repeated experiences of having legitimate emotional reactions dismissed, minimized, or punished prevent the child from learning to identify, label, and regulate their emotional states, leaving them dependent on external validation and unable to self-soothe.
- The transaction: Biological sensitivity provokes intense emotional responses that the environment invalidates, which intensifies the emotional response further, which provokes more invalidation: a developmental transaction that builds toward the explosive reactivity of adult BPD episodes.
Common Interpersonal Triggers for BPD Episodes
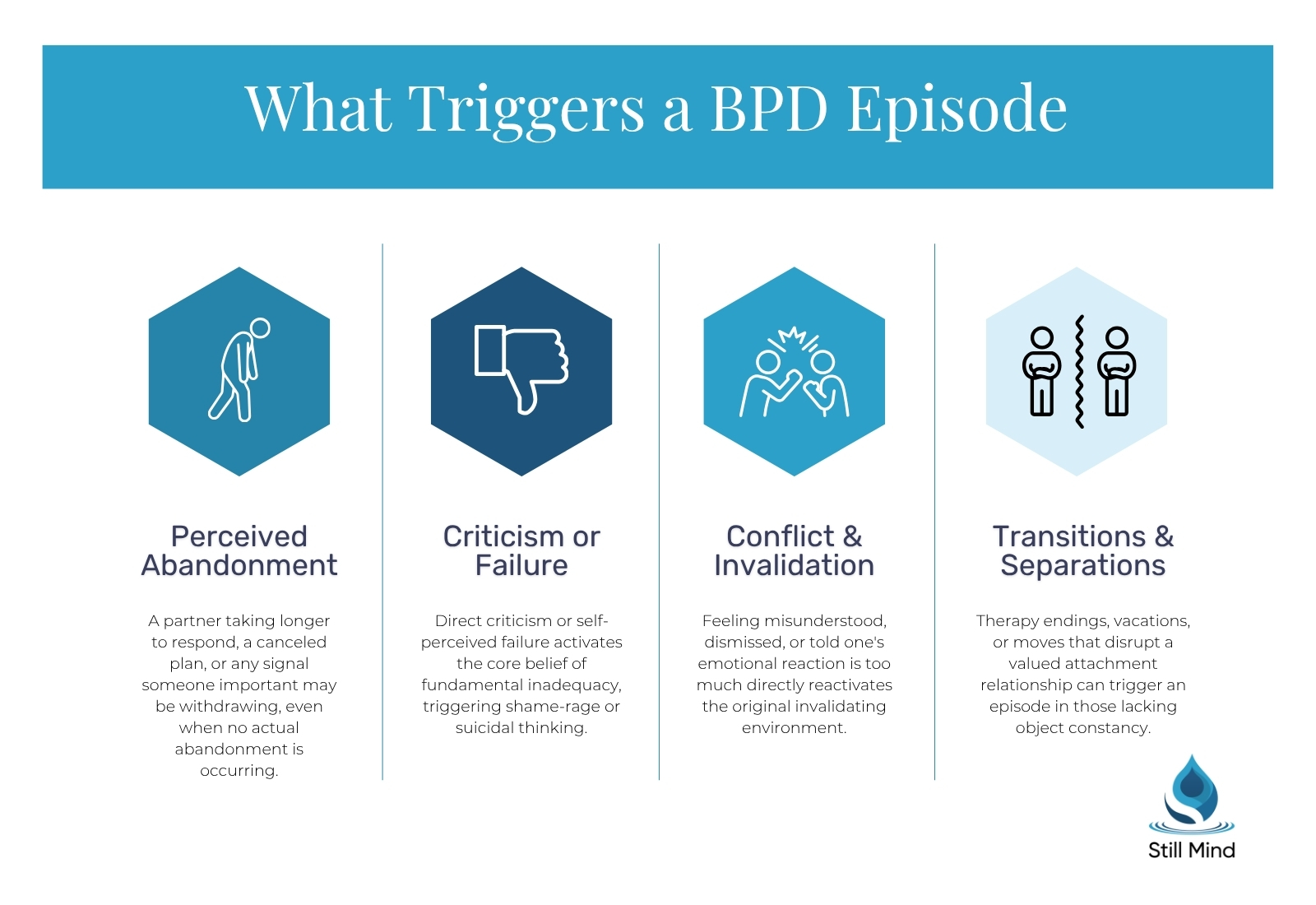
High-risk triggering situations:
- Perceived abandonment or rejection: A partner taking longer than usual to respond to a text, a canceled plan, a change in tone of voice, or any signal that someone important may be withdrawing: even when no actual abandonment is occurring.
- Criticism or perceived failure: Direct criticism, unsolicited feedback, or self-perceived failure at work, school, or relationships activates the internalized belief that the individual is fundamentally inadequate, triggering shame-rage or suicidal thinking.
- Conflict and invalidation: Feeling misunderstood, dismissed, or told that one’s emotional reaction is “too much” directly activates the original invalidating environment that shaped the disorder, generating disproportionate emotional responses to what others view as ordinary disagreements.
- Transitions and separations: Vacations, moving, the end of therapy sessions, graduations, or any transition that disrupts a valued attachment relationship can precipitate an episode, particularly when the individual lacks object constancy: the ability to hold a stable positive internal image of someone when they are absent. Rejection sensitive dysphoria amplifies the pain of these transitions significantly.
How Long Do BPD Episodes Last?
Duration is the single most clinically important feature distinguishing BPD emotional episodes from mood episodes in other psychiatric conditions, particularly bipolar disorder.
Duration by Episode Type
BPD episode duration ranges by type:
- Rage and explosive episodes: Typically 20 minutes to 3 hours; usually resolve once the triggering interaction ends or the individual has physically separated from the situation; longer episodes are associated with ongoing conflict or re-triggering.
- Dissociative episodes: Minutes to several hours in mild presentations; severe episodes involving significant identity disruption can persist through a full day, particularly following major trauma-related triggers or sleep deprivation.
- Suicidal crisis episodes: Acute suicidal crises in BPD often emerge and de-escalate within hours when effectively contained with DBT crisis skills; however, without adequate coping resources or clinical support, these can extend for days and escalate to hospitalization.
- Splitting episodes: The cognitive reorganization of a relationship from idealization to devaluation can lock in for days to weeks, persisting until the individual either repairs the relationship, processes the perceived injury in therapy, or forms a new idealized attachment elsewhere.
What Prolongs a BPD Episode
Factors that extend episode duration and severity:
- Continued exposure to the trigger: Remaining in the interpersonal situation that caused the episode, or continuing to receive messages or calls from the triggering person, prevents the neurobiological de-escalation process from initiating.
- Rumination and self-criticism: Post-episode shame spirals, in which individuals relentlessly analyze what they did wrong or castigate themselves for their reaction, prolong emotional dysregulation well beyond the initial acute phase.
- Substance use: Alcohol and drugs used to numb emotional pain during an episode reduce natural de-escalation, impair judgment, increase impulsivity, and substantially elevate the risk of self-harm and suicidal behavior.
- Sleep deprivation: Insufficient sleep lowers the threshold for amygdala activation, meaning a lower-intensity trigger can produce an episode of equal or greater severity than a higher-intensity trigger during adequate rest.
What Does a BPD Episode Look Like? Signs by Type
From the outside, BPD episodes present a recognizable behavioral signature for each type: though the intensity can be confusing and distressing for family members, partners, and colleagues who observe them without understanding the underlying neurobiology.
Common Signs Across All BPD Episodes
Cross-episode behavioral signs:
- Sudden shift from baseline: A rapid transition from apparent calm or normal functioning to intense emotional distress, often within minutes and in response to a trigger that observers may perceive as minor.
- All-or-nothing framing: Statements that reflect absolute, black-and-white thinking about a person or situation: “you always abandon me,” “nothing ever goes right,” “everyone hates me”: without middle-ground acknowledgment.
- Loss of object constancy: Acting as though past positive experiences with a person have been completely erased by the current triggering event, demanding proof of care that was previously demonstrated repeatedly.
Severe Symptoms and High-Risk Signs Requiring Immediate Response
High-risk behavioral indicators:
- Direct statements of suicidal intent: Any explicit statement of intent to harm oneself requires immediate clinical assessment; in BPD, these statements may be dismissed as “manipulation” but carry genuine suicide risk: individuals with BPD have a lifetime completed suicide rate of approximately 10%.
- Self-harm behaviors: Cutting, burning, hitting, or other forms of self-harm during an episode; while often serving an emotion-regulation function (relieving psychological pain through physical sensation), these behaviors require clinical intervention regardless of stated intent.
- Dissociative disconnection: A glassy, flat affect combined with apparent unawareness of surroundings, inability to respond to questions, or statements like “I can’t feel anything” or “nothing feels real” following extreme emotional escalation.
- Threats toward others: Statements of intent to harm others during rage episodes require immediate safety assessment and may necessitate emergency contact with crisis services or law enforcement.
Long-Term Consequences of Unmanaged BPD Episodes
Chronic impact of untreated episodic dysregulation:
- Relationship deterioration: The combination of rage episodes, splitting, and frantic abandonment behaviors progressively damages relationships even with people who initially have high tolerance, often resulting in the very abandonment the individual feared.
- Occupational impairment: Episodes triggered in work settings: by criticism from supervisors, perceived slights from colleagues, or professional setbacks: can result in impulsive resignations, terminations for conduct, and an inability to sustain long-term employment.
- Escalating self-harm patterns: Without DBT or comparable intervention, self-harm behaviors often escalate in frequency and severity over time as the nervous system habituates to lower-intensity stimulation, requiring increasingly intense behaviors to achieve relief from emotional pain.
How to Get Through a BPD Episode
Evidence-based strategies for managing acute BPD episodes work by targeting the neurobiological systems that drive them: rapidly reducing amygdala activation through physiological means, buying time for the prefrontal cortex to re-engage, and preventing behavioral responses that cause long-term harm.
DBT Distress Tolerance Skills for Acute Episodes
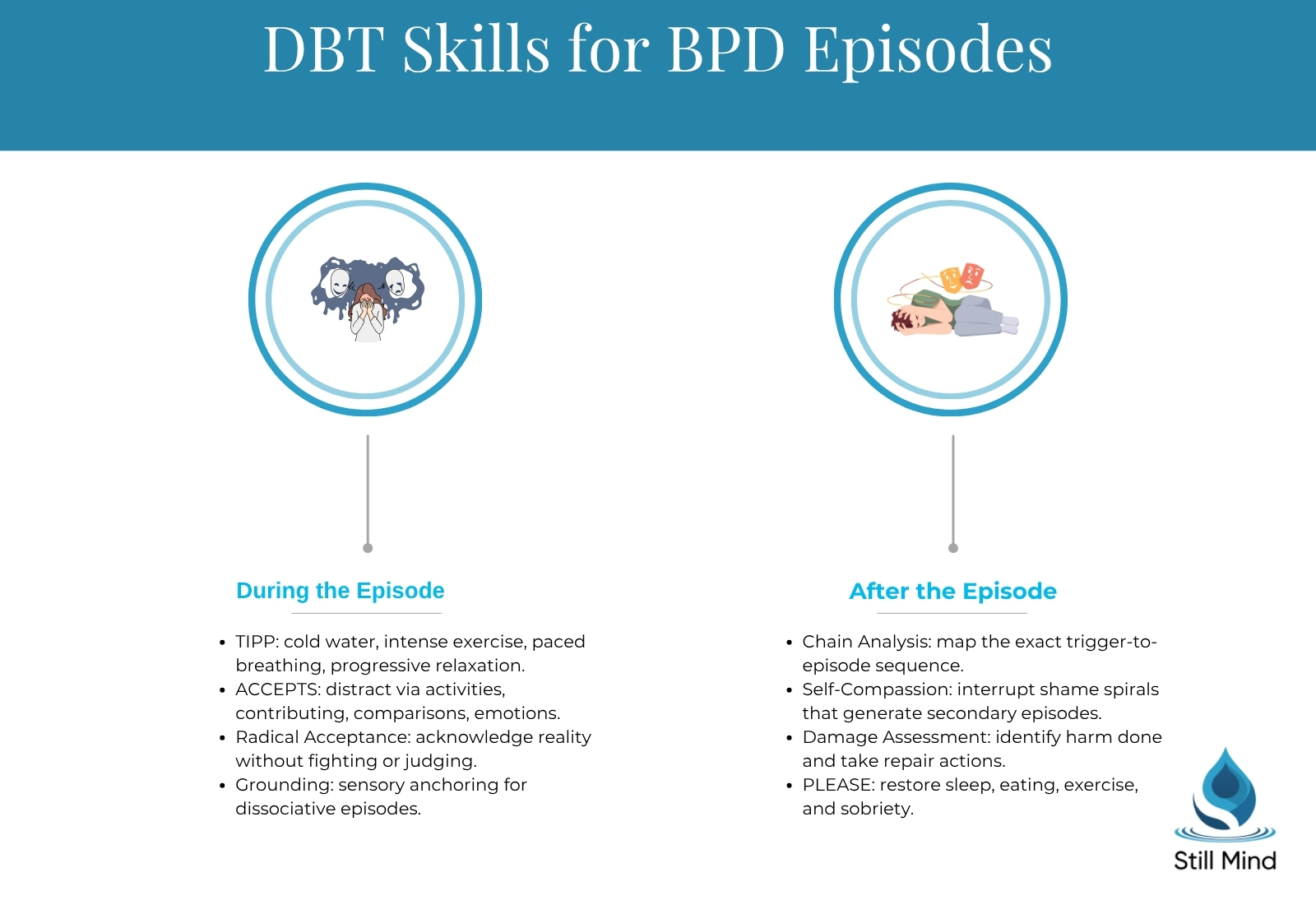
Skills from dialectical behavior therapy for acute crisis moments include:
- TIPP: The TIPP skill targets the Temperature (placing the face in cold water or holding ice to activate the diving reflex, which reduces heart rate and emotional arousal rapidly), Intense exercise (brief burst of physical activity to discharge adrenaline), Paced breathing (extending the exhale to activate the parasympathetic nervous system), and Progressive muscle relaxation (systematically releasing physical tension that amplifies emotional intensity).
- ACCEPTS: A distress tolerance tool that redirects attention away from the triggering stimulus through Activities, Contributing to others, Comparisons to worse situations, contrasting Emotions, Pushing away the situation temporarily, substituting other Sensations, and engaging in distracting Thoughts: designed to bridge the acute crisis period without making it worse.
- Radical acceptance: The DBT skill of fully acknowledging reality as it is without fighting or judging it; during acute episodes, the refusal to accept a triggering reality (a relationship’s limitations, a person’s behavior, one’s own emotional response) intensifies suffering beyond what the situation itself warrants.
Grounding Techniques for Dissociative Episodes
Grounding approaches targeting dissociation specifically:
- Sensory anchoring: Holding ice cubes, touching textured surfaces, smelling strong scents, or tasting something intensely flavored engages present-moment sensory awareness and interrupts the dissociative withdrawal from body and environment.
- Name-five-things grounding: Systematically identifying five visible objects, four touchable surfaces, three sounds, two smells, and one taste progressively re-anchors attention to the immediate environment; this 5-4-3-2-1 technique specifically counters the derealization that accompanies dissociative BPD episodes.
- Rhythmic bilateral stimulation: Slow, alternating tapping on the knees or alternating hand squeezes activates the orienting response and gently re-engages bilateral brain processing disrupted during dissociation.
After the Episode: Making Sense of What Happened
Post-episode processing strategies:
- Chain analysis: A core DBT tool in which the individual maps the precise sequence of events, thoughts, emotions, sensations, and behaviors that led from the triggering event through the peak of the episode to its resolution: identifying specific points where different choices could have produced different outcomes.
- Self-compassionate repair: Post-episode shame is one of the most powerful predictors of subsequent episodes; practicing the same compassionate tone toward oneself that one would offer a friend in the same situation interrupts shame-driven self-criticism that produces secondary emotional cycles.
- Damage assessment and repair: Identifying any relationships or situations damaged during the episode and taking repair actions once regulated: not during the episode itself, when apologies and repairs are often followed quickly by new escalation.
“Most patients who come to us during a BPD crisis have spent years being told their reactions are ‘too much.’ What DBT actually does is give them a language for what’s happening neurobiologically and tools that work with that biology rather than asking them to simply stop feeling. Within days, most patients can identify their specific triggers and apply at least one distress tolerance skill before the episode peaks: and that’s a genuinely significant change.”
– Dr. Gladys Martinez
Treatment for BPD Episodes at Still Mind
Still Mind provides specialized treatment for borderline personality disorder that addresses both the neurobiological vulnerabilities driving BPD episodes and the interpersonal and behavioral patterns that maintain them.
Dialectical Behavior Therapy
DBT at Still Mind include:
- Evidence base: DBT is the gold-standard treatment for BPD, with randomized controlled trials demonstrating significant reductions in self-harm frequency, suicidal behavior, psychiatric hospitalizations, and treatment dropout compared to standard community care.
- Skill modules targeting episodes: The distress tolerance module specifically addresses acute BPD episodes by providing practical, neurobiologically grounded tools for surviving crisis without making behaviors worse; emotion regulation skills address the between-episode vulnerability that determines how quickly an individual reaches the episode threshold.
- Individual and skills training components: Still Mind’s DBT program provides both the individual therapy component: where therapists help patients apply skills to specific real-life situations using chain analysis: and the skills training component where the four DBT modules are taught systematically.
Mentalization-Based Therapy and Cognitive Behavioral Therapy
MBT as a second-line evidence-based approach:
- What mentalization targets: Mentalization-based therapy, developed by Dr. Peter Fonagy and Dr. Anthony Bateman, addresses the core deficit in BPD that underlies episodes: the temporary collapse of mentalizing: the capacity to understand one’s own and others’ behavior in terms of mental states: under emotional arousal.
- Clinical mechanism: MBT produces reductions in BPD episode frequency by specifically rebuilding the mentalizing capacity that breaks down during acute interpersonal triggers, strengthening the patient’s ability to consider alternative explanations for others’ behavior before reaching a BPD-episode-generating conclusion about abandonment or rejection.
Dual Diagnosis Treatment
Comorbidity management:
- Comorbidity burden in BPD: Approximately 80% of individuals with BPD meet diagnostic criteria for at least one comorbid condition, with major depressive disorder, PTSD, anxiety disorders, and substance use disorders being most common; each comorbidity lowers the threshold for BPD episodes by increasing overall emotional arousal.
- Integrated treatment: Dual diagnosis treatment addresses co-occurring substance use and BPD simultaneously, recognizing that substance use both increases BPD episode frequency and severity and complicates the safety picture during suicidal or self-harm crises.
To discuss treatment options for BPD episodes at Still Mind, contact the admissions team directly for a confidential assessment.
Frequently Asked Questions
What is a BPD episode?
A BPD episode is an acute period of intense emotional dysregulation in borderline personality disorder, typically triggered by a perceived interpersonal threat and characterized by rage, dissociation, suicidal urges, or a collapse of self-image. Unlike a bipolar mood episode, a BPD episode is reactive to a specific trigger and typically resolves within hours rather than days or weeks. The term is not a formal DSM-5-TR category but describes the recognizable pattern of acute emotional crises that define BPD’s clinical course.
What does a BPD episode feel like?
Individuals with BPD describe episodes as feeling like “being on fire from the inside,” losing all access to the rational part of their mind, seeing the world in absolute black-and-white terms, and feeling either overwhelmingly flooded with emotion or completely numb and disconnected. Physical sensations commonly include racing heart, chest tightness, shaking, and a sense of unreality. The experience is qualitatively different from ordinary sadness or anger: the intensity is neurobiologically driven by amygdala hyperreactivity that produces emotional responses that feel entirely beyond voluntary control.
How long do BPD episodes last?
Most acute BPD episodes resolve within minutes to several hours, though this varies by episode type. Rage episodes typically last 20 minutes to 3 hours; dissociative episodes can last minutes to a full day. Suicidal crises without clinical support may extend for days. The splitting-triggered collapse of a relationship from idealization to devaluation can persist for days to weeks. Duration is the key clinical differentiator from bipolar disorder: bipolar manic episodes require at least 7 days for diagnosis, while BPD emotional shifts resolve far more rapidly.
What triggers a BPD episode?
BPD episodes are almost always triggered by interpersonal events: perceived abandonment, rejection, criticism, invalidation, or conflict with someone the individual has a strong attachment to. Transitions and separations, including the end of a therapy session, also function as triggers. Physical vulnerabilities: sleep deprivation, hunger, illness, and substance use: lower the threshold at which a triggering event produces a full episode. The trigger does not need to be objectively significant; the amygdala hyperreactivity in BPD detects threat in neutral social stimuli that most people would not register.
What happens after a BPD episode?
Post-episode experience varies by individual but commonly includes intense shame and regret, exhaustion, relief that the acute distress has passed, and fear about what was said or done during the episode and its consequences for relationships. Many individuals with BPD experience a secondary wave of emotional dysregulation driven by shame-based self-criticism about the episode itself. Therapy-focused post-episode chain analysis: identifying the exact sequence of events that led to the episode: is the most clinically valuable activity after the acute phase has resolved.
Is a BPD episode the same as a bipolar episode?
No. BPD episodes and bipolar mood episodes differ fundamentally in duration, triggers, and neurobiological mechanism. BPD emotional episodes last minutes to hours and are triggered by specific interpersonal events; bipolar mood episodes last days to weeks and often arise without an identifiable external trigger. BPD episodes involve the reactive emotional system governed by the amygdala; bipolar episodes involve a fundamental state shift in neurobiological systems governing mood across the full circadian cycle. Both conditions involve emotional intensity, which creates frequent diagnostic confusion, but they require different treatments.
Can BPD episodes be prevented?
BPD episodes cannot be eliminated, particularly early in treatment, but their frequency, intensity, and consequences can be substantially reduced through DBT and related evidence-based therapies. DBT specifically targets both the immediate episode (through crisis survival skills) and the vulnerability state that determines how easily a trigger produces an episode (through emotion regulation and PLEASE skills targeting physical health, sleep, and substance use). After adequate DBT participation, most patients report significantly fewer episodes, improved ability to apply skills before the episode peaks, and reduced reliance on self-harm as a coping strategy.
What should you NOT say during a BPD episode?
Statements that invalidate the emotional experience (“you’re overreacting,” “this is nothing to cry about,” “you’re being dramatic”) escalate rather than de-escalate BPD episodes, directly replicating the invalidating environment that shaped the disorder. Ultimatums, threats to end the relationship, or withdrawing physically without explanation also intensify abandonment-triggered episodes. The most effective de-escalation approach involves validating the emotional experience without endorsing the catastrophic interpretations, maintaining calm presence, and avoiding power struggles about the accuracy of the person’s perceptions during the acute crisis.
References
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (DSM-5-TR). American Psychiatric Publishing.
- Linehan, M. M. (1993). Cognitive-behavioral treatment of borderline personality disorder. Guilford Press.
- Zanarini, M. C., Frankenburg, F. R., Hennen, J., Reich, D. B., & Silk, K. R. (2006). Prediction of the 10-year course of borderline personality disorder. American Journal of Psychiatry, 163(5), 827–832.
- National Alliance on Mental Illness. (2024). Borderline personality disorder: Prevalence and clinical features. https://www.nami.org
- Trull, T. J., Lane, S. P., Koval, P., & Ebner-Priemer, U. W. (2019). Affective dynamics in psychological science. Perspectives on Psychological Science, 10(4), 512–536.
- National Institute of Mental Health. (2024). Borderline personality disorder. https://www.nimh.nih.gov/health/topics/borderline-personality-disorder
- Fonagy, P., & Bateman, A. (2016). Mechanisms of change in mentalization-based treatment of BPD. Journal of Clinical Psychology, 62(4), 411–430.
- Substance Abuse and Mental Health Services Administration. (2023). National survey on drug use and health: Key substance use and mental health indicators. https://www.samhsa.gov