




Quiet BPD represents a manifestation of borderline personality disorder where symptoms are directed inward rather than expressed through dramatic outbursts or external volatility.
Unlike the stereotypical image of BPD involving explosive relationships and visible emotional chaos, individuals with quiet BPD experience the same core symptoms of emotional dysregulation, fear of abandonment, and unstable self-image as internal suffering.
This internalized form of borderline personality disorder creates a paradox where people appear highly functional on the surface while experiencing intense emotional turmoil privately. They turn their pain inward through self-blame, withdrawal, perfectionism, and hidden self-destructive behaviors rather than acting out against others. The hidden nature of quiet BPD makes it particularly challenging to recognize and diagnose, often leaving individuals struggling alone for years without proper support or treatment.
So why do some people with borderline personality disorder suffer in silence while others display their symptoms more openly?
Key Takeaways
- Quiet BPD, also known as the “discouraged” subtype of borderline personality disorder, affects individuals who direct their emotional dysregulation inward through self-blame, withdrawal, and perfectionism rather than external acting out.
- The National Institute of Mental Health recognizes that borderline personality disorder affects a significant portion of U.S. adults, with many cases going undiagnosed due to the hidden nature of quiet presentations.
- People with quiet BPD often appear high-functioning and successful in their careers and relationships while experiencing severe internal emotional instability, chronic emptiness, and fear of abandonment.
- The Substance Abuse and Mental Health Services Administration emphasizes that dialectical behavior therapy remains the gold standard treatment for all BPD subtypes, including quiet presentations.
- Early recognition and intervention significantly improve long-term outcomes, with research showing substantial symptom reduction when individuals receive appropriate trauma-informed treatment.
What Is Quiet BPD and Why Is It So Hard to Recognize?
Quiet borderline personality disorder represents what clinicians classify as the “discouraged” subtype of BPD, characterized by the internalization of emotional dysregulation rather than its external expression.
The National Institute of Mental Health identifies borderline personality disorder as a serious mental health condition affecting a substantial portion of adults in the United States. Many cases involving quiet presentations remain undiagnosed because symptoms manifest as self-directed criticism, emotional withdrawal, people-pleasing behaviors, and hidden self-destructive patterns.
The core features of BPD remain unchanged in quiet presentations: intense fear of abandonment, unstable interpersonal relationships, identity disturbance, impulsivity, emotional instability, chronic emptiness, inappropriate anger, and stress-related dissociation. Recognition becomes challenging because individuals with quiet BPD develop sophisticated masking strategies to hide their internal chaos.
They may excel professionally, maintain long-term relationships, and appear emotionally stable while privately experiencing intense emotional storms, overwhelming shame, and persistent suicidal ideation. The diagnostic complexity of BPD increases when considering that many people with quiet BPD receive misdiagnoses of depression, anxiety disorders, or bipolar disorder before the underlying personality structure becomes apparent. BPD is diagnosed by the BPD test, helping individuals to understand their feelings and emotions better.
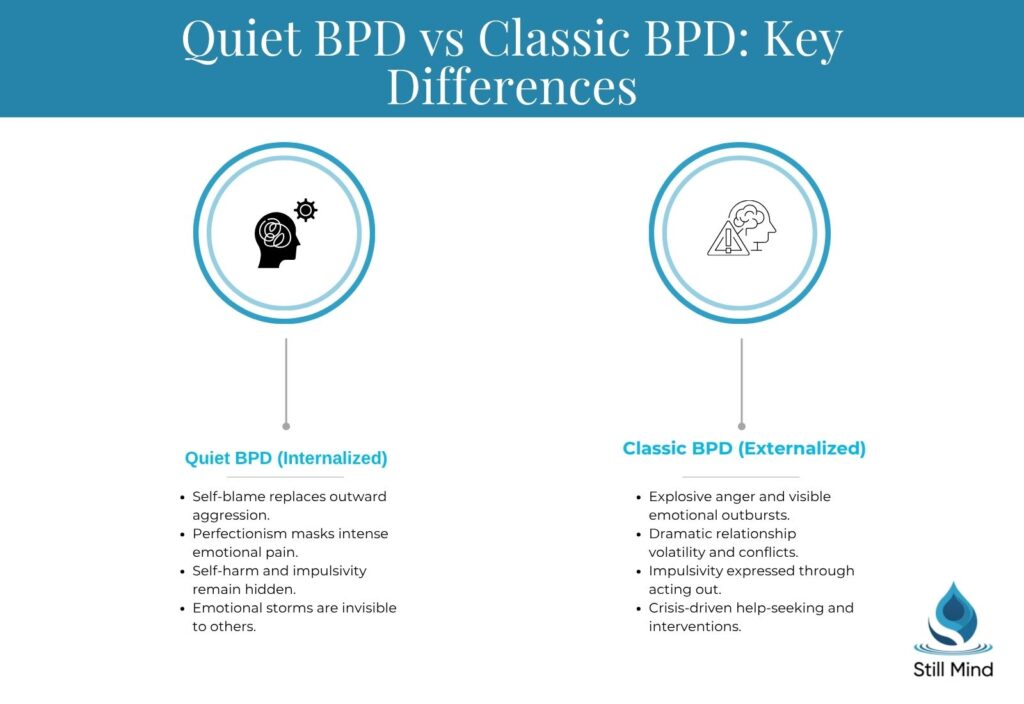
How Does Quiet BPD Differ from Classic BPD?
| Symptom Category | Classic BPD | Quiet BPD |
|---|---|---|
| Emotional Expression | Outward volatility, explosive anger | Internal emotional storms, self-directed rage |
| Relationship Patterns | Dramatic conflicts, visible push-pull dynamics | Secret resentment, silent withdrawal |
| Coping Mechanisms | External acting out, substance abuse | Self-blame, perfectionism, hidden self-harm |
| Help-Seeking Behavior | Crisis-driven, emergency interventions | Delayed seeking, masking distress |
| Self-Image | Unstable but expressed openly | Chronic shame, impostor syndrome |
The fundamental difference lies in the direction of symptom expression rather than their underlying intensity or severity.
What Are the Hidden Signs of Quiet BPD?
The American Psychiatric Association’s DSM-5-TR criteria for borderline personality disorder manifest uniquely in quiet presentations.
Recognition requires understanding how each criterion appears when directed inward rather than expressed externally. Clinicians must look beneath the surface of apparent functioning to identify these internalized patterns. The symptoms create persistent internal distress while maintaining external competence, creating a complex diagnostic challenge.
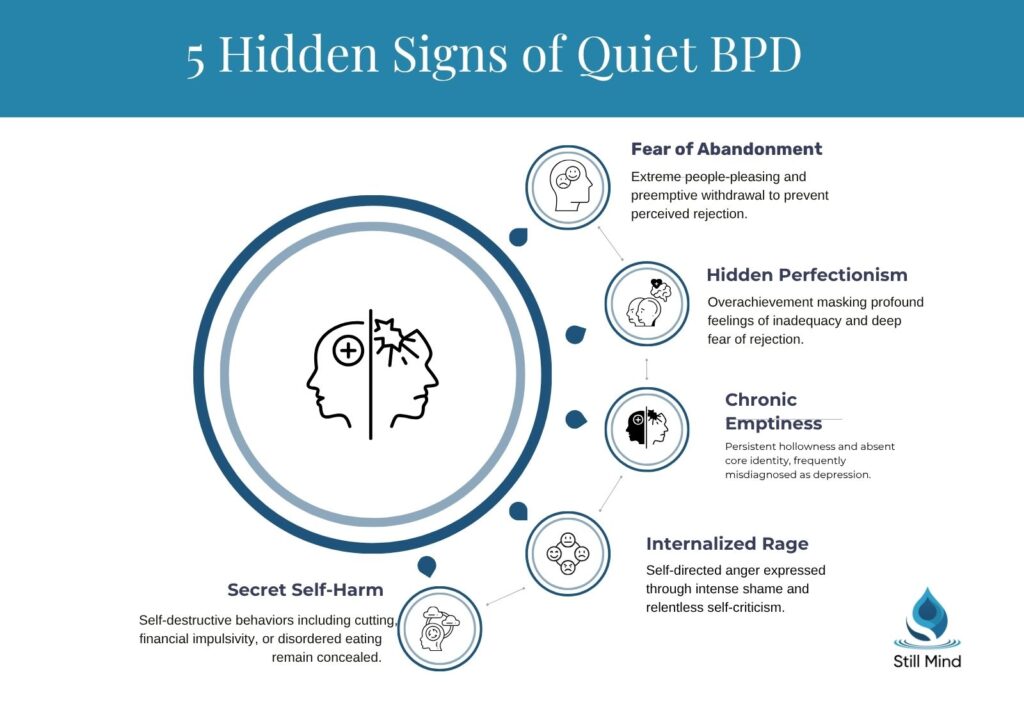
Fear of Abandonment
- Excessive people-pleasing: Going to extreme lengths to avoid conflict or disagreement
- Over-apologizing: Constant apologies for normal behavior or perceived slights
- Hypervigilance to rejection: Scanning for signs of disapproval or withdrawal in others
- Preemptive withdrawal: Ending relationships before being abandoned
Unstable Relationships
- Idealization followed by secret resentment: Putting others on pedestals then privately criticizing them
- Emotional unavailability: Maintaining surface-level connections while feeling disconnected
- Difficulty with intimacy: Fear of being truly known or seen
- Caretaking patterns: Focusing on others’ needs while neglecting their own
Identity Disturbance
- Chronic emptiness: Persistent feelings of hollowness or lacking a core self
- Impostor syndrome: Feeling fraudulent despite external achievements
- Values confusion: Uncertainty about personal beliefs, goals, or preferences
- Role-dependent identity: Defining themselves entirely through relationships or achievements
Hidden Impulsivity and Self-Harm
- Financial impulsivity: Hidden spending sprees or financial self-sabotage
- Eating behaviors: Binge eating, restriction, or other disordered patterns
- Self-harm: Cutting, burning, or other forms of self-injury done in private
- Sexual behaviors: Risky sexual encounters or sexual self-harm
Why Do People with Quiet BPD Appear High-Functioning?
High functioning BPD creates a deceptive external presentation that masks profound internal suffering.
Individuals develop sophisticated compensatory mechanisms including:
- Perfectionism
- Overachievement
- Meticulous self-control that allows them to maintain jobs, relationships, and social obligations
- Severe emotional dysregulation privately.
The perfectionist drive often stems from deep shame and fear of rejection, creating a relentless pursuit of external validation through achievement.
These individuals may excel in demanding careers, maintain immaculate living spaces, and present themselves as highly competent while internally struggling with overwhelming feelings of inadequacy and emptiness. People-pleasing behaviors become another layer of the high-functioning mask, as they prioritize others’ needs and emotions above their own to maintain relationships and avoid abandonment.
This pattern creates exhaustion from constant emotional monitoring and self-suppression, yet the external observer sees someone who appears exceptionally caring and selfless. The energy required to maintain this facade eventually leads to periodic breakdowns, often misinterpreted as isolated episodes of depression or anxiety rather than manifestations of an underlying personality disorder. The contrast between their public competence and private struggles contributes to delayed diagnosis and treatment, as both the individual and clinicians may focus on treating symptoms rather than addressing the core emotional dysregulation.
How Can You Tell If You Might Have Quiet BPD?
Self-assessment for quiet BPD requires honest examination of internal experiences that may never have been shared with others.
The following framework helps identify potential symptoms across three severity levels, though professional evaluation remains essential for accurate diagnosis. Understanding these patterns can help determine when to seek professional support and what information to share with mental health providers.

Mild Presentations
Occasional people-pleasing that feels automatic, heightened sensitivity to criticism or rejection, and periods of feeling emotionally empty or disconnected. These symptoms may be attributed to stress or personality traits rather than recognized as part of a pattern.
Action steps: Begin practicing emotional awareness through journaling, notice patterns in relationships and self-criticism, and consider whether these experiences significantly impact daily functioning.
Moderate Presentations
Chronic self-doubt despite external achievements, regular emotional episodes managed privately, persistent fear of abandonment affecting relationship choices, and hidden self-destructive behaviors like overspending or self-harm.
Work and relationship functioning remain intact but require significant emotional energy to maintain. Action steps: Schedule consultation with a mental health professional experienced in personality disorders, begin tracking mood patterns and triggers, and consider whether current coping strategies create long-term problems.
Severe Presentations
Constant internal criticism, frequent dissociative episodes, severe emotional instability hidden from others, regular self-harm or suicidal ideation, and complete emotional shutdown in response to stress. Despite maintaining external functioning, internal suffering becomes overwhelming and unsustainable.
Action steps: Seek immediate professional evaluation from a trauma-informed clinician specializing in personality disorders, develop safety plans for self-harm urges, and consider intensive treatment options if symptoms significantly impair functioning.
What Treatment Options Work Best for Quiet BPD?
Evidence-based treatments for quiet borderline personality disorder focus on developing emotional regulation skills, building distress tolerance, and addressing underlying trauma patterns. The Substance Abuse and Mental Health Services Administration emphasizes that specialized therapy approaches show significantly better outcomes than general counseling for personality disorder presentations. Treatment often requires longer therapeutic engagement than classic presentations, as individuals need time to build trust before revealing internal experiences honestly.
Psychotherapy Approaches
- Dialectical Behavior Therapy (DBT): The gold standard treatment for quiet BPD, DBT teaches concrete skills for managing emotional intensity, improving interpersonal effectiveness, and replacing self-destructive behaviors with healthier distress tolerance strategies.
- Cognitive Behavioral Therapy (CBT): CBT targets the negative thought patterns and internalized shame that sustain quiet BPD symptoms, helping individuals recognize distorted thinking and develop more balanced self-perception.
- Mentalization-Based Treatment (MBT): Specifically addresses the difficulty understanding one’s own and others’ mental states, a core challenge in BPD that often drives emotional misreads and relationship strain.
Medication and Combined Care
- Psychiatric Medication: Does not treat core personality disorder symptoms but can stabilize co-occurring depression, anxiety, or mood instability when clinically indicated.
- Combined Treatment Approach: The most effective outcomes result from pairing evidence-based psychotherapy with targeted medication management, particularly for individuals with significant mood or anxiety symptoms alongside BPD.
What Are the Long-Term Outcomes for Quiet BPD?
Recovery from quiet BPD shows promising outcomes with specialized treatment. Clinical studies show that a significant majority of individuals no longer meet full diagnostic criteria after extended follow-up periods. Quiet BPD prognosis is often favorable, as these individuals typically bring strong motivation and existing coping skills into treatment.
Positive Recovery Indicators
- Symptom Reduction Over Time: A significant majority of individuals with BPD no longer meet full diagnostic criteria after extended follow-up with appropriate treatment.
- Strong Treatment Motivation: High internal drive for change supports sustained therapeutic engagement and faster progress.
- Functional Stability: Maintained daily functioning during treatment provides a stable base for deeper therapeutic work.
Risks of Untreated Quiet BPD
- Chronic Mental Health Conditions: Untreated quiet BPD increases risk of persistent depression and anxiety disorders.
- Relationship Difficulties: Emotional suppression and internalized shame create recurring cycles of withdrawal and disconnection.
- Increased Suicide Risk: Sustained emotional masking elevates long-term suicide risk as symptom burden accumulates.
- Burnout and Escalation: Maintaining a high-functioning facade depletes psychological resources, leading to burnout and more severe presentations over time.
Treatment for Quiet Borderline Personality Disorder
Effective treatment for quiet BPD requires specialized approaches that address both the internalized nature of symptoms and the underlying emotional dysregulation.
Mental health facilities offering comprehensive personality disorder treatment provide the structured environment necessary for developing new coping strategies and processing underlying trauma.
Dialectical Behavior Therapy (DBT)
Our dialectical behavior therapy program specifically addresses the core symptoms of quiet BPD through skills-based learning in four key areas: mindfulness, distress tolerance, emotion regulation, and interpersonal effectiveness.
DBT’s structured approach proves particularly beneficial for individuals who have learned to suppress rather than express their emotional experiences.
Residential Mental Health Treatment
For individuals with severe quiet BPD symptoms, residential mental health treatment provides intensive therapeutic support in a controlled environment.
This level of care allows for comprehensive assessment, medication stabilization, and intensive therapy while maintaining safety during the initial stages of treatment.
Dual Diagnosis Treatment
Many individuals with quiet BPD also struggle with co-occurring mental health conditions such as depression, anxiety, or substance use disorders.
Dual diagnosis treatment addresses these interconnected conditions simultaneously, recognizing that untreated personality disorder symptoms often contribute to other mental health challenges. Professional evaluation and specialized treatment can provide significant relief and improved functioning for individuals with quiet BPD. The internal suffering associated with quiet BPD responds well to appropriate therapeutic intervention when individuals have access to knowledgeable, trauma-informed care.
The Bottom Line
Quiet BPD represents a significant but often overlooked presentation of borderline personality disorder that requires specialized recognition and treatment approaches. While individuals with this condition may appear highly functional externally, they experience the same intensity of emotional dysregulation and interpersonal difficulties as those with classic BPD presentations, but directed inward rather than expressed outwardly.
The key to addressing quiet BPD lies in recognizing that external functioning does not indicate internal wellness, and that the hidden nature of symptoms often delays crucial treatment interventions. Professional evaluation by clinicians experienced in personality disorder assessment remains essential for accurate diagnosis and appropriate treatment planning. With proper therapeutic support, individuals with quiet BPD can develop healthier emotional regulation strategies, build authentic relationships, and reduce the exhausting effort required to maintain their high-functioning facade.
For those seeking comprehensive mental health treatment that addresses the complex needs of personality disorders, specialized programs provide the structured support necessary for meaningful recovery and long-term emotional stability.
Frequently Asked Questions
What are quiet BPD symptoms?
Quiet BPD symptoms include internalized emotional dysregulation, chronic feelings of emptiness, fear of abandonment expressed through people-pleasing, hidden self-harm behaviors, perfectionism, intense self-criticism, and difficulty maintaining a stable sense of identity. Unlike classic BPD, these symptoms are directed inward rather than expressed through external conflicts or dramatic relationship patterns. These individuals often experience overwhelming shame and engage in secretive self-destructive behaviors while maintaining an appearance of emotional stability to others.
Can you have BPD without dramatic outbursts?
Quiet BPD represents a valid manifestation of borderline personality disorder where individuals experience the same core symptoms without external emotional volatility. These individuals direct their emotional dysregulation inward through self-blame, withdrawal, and hidden self-destructive behaviors rather than explosive interpersonal conflicts. The American Psychiatric Association’s diagnostic criteria for BPD do not require outward emotional displays, recognizing that symptoms can manifest in various ways depending on individual coping patterns and environmental factors.
How is quiet BPD diagnosed by professionals?
Mental health professionals diagnose quiet BPD using the same DSM-5-TR criteria as classic BPD, but look for internalized manifestations of each symptom. Diagnosis requires comprehensive clinical assessment including detailed personal history, symptom patterns, relationship functioning, and screening for co-occurring conditions that may mask personality disorder features. Clinicians examine how fear of abandonment, identity disturbance, emotional instability, and other core symptoms appear when directed inward rather than expressed externally. The process often involves multiple sessions to build trust and reveal hidden symptoms.
What triggers quiet BPD episodes?
Common triggers include perceived rejection or criticism, relationship conflicts, feeling misunderstood or invalidated, major life transitions, stress at work or school, and situations that activate abandonment fears. Unlike classic BPD, episodes may be completely hidden from others, manifesting as internal emotional storms, dissociation, or increased self-destructive behaviors. Triggers often involve subtle social cues that others might not notice, such as changes in tone of voice or delayed responses to messages, which activate deep-seated fears of being unwanted or rejected.
Is quiet BPD easier to treat than classic BPD?
Treatment outcomes depend more on individual factors than BPD subtype, though quiet BPD may present unique advantages and challenges. These individuals often possess strong motivation and coping skills but may struggle with emotional awareness and therapeutic trust. Treatment typically requires longer engagement to address ingrained patterns of emotional suppression and may involve additional work on developing the ability to identify and express emotions safely. The tendency to minimize their own suffering can initially complicate the therapeutic process.
Can quiet BPD develop into classic BPD over time?
BPD presentations can shift based on life circumstances, stress levels, and coping resources. Some individuals with quiet presentations may develop more externalized symptoms during periods of severe stress or trauma, while others maintain consistent internalized patterns throughout their lives. Both presentations represent the same underlying condition with different expression patterns. Environmental factors, relationship dynamics, and available support systems can influence whether symptoms remain internalized or begin manifesting externally over time.
How can family members support someone with quiet BPD?
Family support involves learning about BPD symptoms, avoiding invalidation of emotions, setting healthy boundaries, encouraging professional treatment, and understanding that external functioning does not indicate internal wellness. Family therapy or education programs can help relatives develop effective communication strategies and reduce unintentional triggers. It’s important to validate their internal experiences even when they appear capable and successful externally, and to recognize that their perfectionism or people-pleasing behaviors may mask significant emotional distress.
What should you not say to someone with quiet BPD?
Avoid minimizing statements like “you seem fine,” “just think positive,” or “others have it worse.” Don’t dismiss their internal experiences based on external appearance, pressure them to “open up” before they’re ready, or make their emotional needs about your discomfort. Validation and patience support their healing process more effectively than advice or comparisons. Statements that question the validity of their struggles based on their apparent success can reinforce their tendency to hide emotional pain and delay seeking appropriate help.
References
- American Psychiatric Association. (2024). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). https://www.psychiatry.org
- National Institute of Mental Health. (2024). Borderline personality disorder. https://www.nimh.nih.gov
- Substance Abuse and Mental Health Services Administration. (2024). Treatment approaches for borderline personality disorder. https://www.samhsa.gov