



")
Oppositional defiant disorder (ODD) is a childhood behavioral condition marked by a persistent pattern of angry outbursts, defiant behavior, and vindictiveness toward authority figures. It goes beyond the occasional stubbornness every child shows.
When defiant behavior lasts more than six months and disrupts daily life at home, school, or with peers, it may point to ODD. Early recognition and structured treatment can significantly improve long-term outcomes for children and families.
Highlights
- Oppositional defiant disorder affects an estimated 2% to 11% of children, with a pooled prevalence of approximately 3.6% up to age 18 (American Academy of Family Physicians, 2016).
- Nearly 40% of children diagnosed with ADHD also meet criteria for ODD or a related conduct disorder (Cleveland Clinic, 2022).
- ODD symptoms fall into three DSM-5 categories: angry or irritable mood, argumentative or defiant behavior, and vindictiveness.
- Without proper diagnosis and treatment, ODD behaviors can persist into adulthood and increase the risk of mood disorders and substance use.
- Parent management training is the most evidence-based first-line treatment for ODD, especially in younger children.
What Is Oppositional Defiant Disorder?
Oppositional defiant disorder is a disruptive behavior disorder primarily involving difficulties regulating emotions and behaviors. The DSM-5-TR defines it as a recurrent pattern of negative, defiant, and hostile behavior directed at caregivers, teachers, or other authority figures.
Unlike typical childhood defiance, ODD behaviors are persistent, excessive for the child’s developmental level, and cause significant impairment. Symptoms must be present for at least six months and occur with at least one person who is not a sibling.
ODD is most often diagnosed in childhood, but can be identified and treated in adults as well. Boys are diagnosed at slightly higher rates than girls, and prevalence generally declines with increasing age.
ODD Symptoms: The 3 DSM-5 Categories
To meet criteria for ODD, the DSM-5-TR requires at least four symptoms from any of the three categories below. These symptoms must occur frequently, cause impairment in functioning, and be observed across multiple settings.
1. Angry or Irritable Mood
- Frequent loss of temper
- Being easily annoyed or touchy
- Often appearing angry and resentful
2. Argumentative or Defiant Behavior
- Frequently argues with adults or authority figures
- Actively refuses to follow rules or comply with requests
- Deliberately annoys or provokes others
- Blames others for their own mistakes or misbehavior
3. Vindictiveness
- Has been spiteful or vindictive at least twice in the past six months
- Seeks revenge or retaliation after perceived slights
Symptoms often appear most strongly at home but can show up at school and in social settings. The DSM-5 also specifies severity levels: mild (symptoms in one setting), moderate (symptoms in two settings), or severe (symptoms in three or more settings).
What Causes Oppositional Defiant Disorder?
ODD has no single confirmed cause. Research consistently points to a combination of biological, genetic, and environmental factors that interact over time.
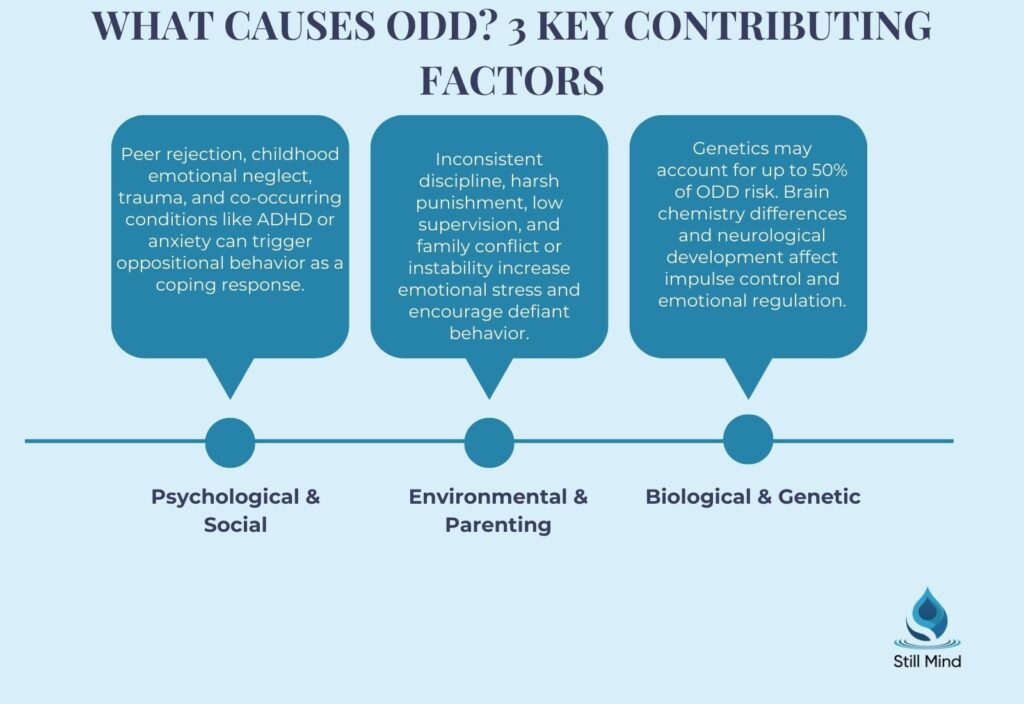
Biological and Neurological Factors
Disruptions in neurotransmitter regulation, particularly in dopamine and serotonin systems, are associated with the mood and impulse control difficulties seen in ODD. Some children show differences in brain structure and function in areas governing emotional regulation and decision-making.
Children with emotional dysregulation as an early trait are at higher risk of developing ODD, particularly when environmental stressors are also present.
Genetic Factors
ODD has a heritable component. Children are at elevated risk when a parent has a history of ODD, ADHD, or other behavioral or mood disorders. Twin studies suggest moderate genetic contributions, though no single gene has been identified.
Environmental and Family Factors
Inconsistent discipline, harsh parenting, family instability, and a chaotic home environment all increase risk. Childhood emotional neglect is closely linked to difficulties with emotional regulation and compliance in early development.
Socioeconomic stress, peer conflict, and exposure to violence also contribute. The developmental theory of ODD suggests some children struggle to individuate appropriately from caregivers during toddlerhood, with defiance persisting beyond normal developmental stages.
ODD in Children vs. ODD in Adults
ODD is primarily diagnosed in childhood, but a significant number of cases persist into adolescence and adulthood. The presentation can shift over time.
| Feature | ODD in Children | ODD in Adults |
|---|---|---|
| Primary targets | Parents, teachers, caregivers | Bosses, partners, law enforcement |
| Common triggers | Rules, homework, bedtime routines | Workplace demands, authority figures |
| Comorbidities | ADHD, learning disorders, anxiety | Depression, personality disorders, substance use |
| Diagnosis complexity | Easier to identify via behavior reports | Often misidentified as personality disorder |
| Treatment approach | Parent management training, CBT, school intervention | Individual therapy, DBT, anger management |
Adults with undiagnosed ODD often have a long history of interpersonal conflict, job instability, and strained relationships. They may not recognize their own behavior as defiant, instead viewing authority as unfair or unjust.
How Is ODD Diagnosed?
There are no laboratory tests or imaging studies required to diagnose oppositional defiant disorder. Diagnosis is clinical and based on DSM-5-TR criteria.
A qualified mental health professional will conduct a comprehensive evaluation that includes interviews with the child, parents, and often teachers. They will assess the frequency, severity, and duration of symptoms, as well as the settings in which they occur.
Clinicians also screen for co-occurring conditions, including ADHD, anxiety, depression, learning disorders, and language disabilities. Accurately ruling out or confirming comorbidities is essential for building an effective treatment plan.
Symptoms must be present for at least six months and occur at a rate greater than what is typically seen in peers of the same age, culture, and developmental level. For children under five, the behavior must occur on most days.
ODD vs. Conduct Disorder: Key Differences
About 30% of children with ODD go on to develop conduct disorder (CD), a more severe disruptive behavior disorder. Understanding the distinction matters for treatment planning and long-term prognosis.
| Feature | Oppositional Defiant Disorder | Conduct Disorder |
|---|---|---|
| Core behavior | Defiance, anger, vindictiveness | Aggression, rule violations, antisocial acts |
| Rule violations | Refusing or arguing against rules | Actively breaking rules and laws |
| Harm to others | Emotionally, through provocation | Physical, through violence or cruelty |
| Property damage | Not a defining feature | Stealing, vandalism, destruction |
| Long-term risk | Conduct disorder, mood disorders | Antisocial personality disorder, incarceration |
| DSM-5 classification | Separate from CD; not an exclusion criterion | More severe diagnosis on the spectrum |
Children who show symptoms of both conditions, combined with patterns of rule-breaking and aggression, should be evaluated for antisocial personality disorder risk factors as they move into adolescence.
ODD and Comorbidities
ODD rarely occurs in isolation. The majority of children with this diagnosis also have at least one co-occurring condition. Identifying and treating comorbidities is central to effective management.
Common co-occurring conditions include:
- ADHD: The most frequent comorbidity; children with both ADHD and ODD typically show more aggression and greater academic impairment.
- Anxiety disorders: Up to 50% of individuals with ODD have comorbid anxiety or depression, according to research cited by the American Academy of Family Physicians.
- Depressive disorders: Particularly in older children and adolescents, the irritability dimension of ODD overlaps significantly with mood dysregulation.
- Disruptive mood dysregulation disorder (DMDD): Shares features with ODD but involves severe, recurrent temper outbursts. Understanding disruptive mood dysregulation disorder helps clinicians differentiate the two diagnoses accurately.
- Learning disabilities: Academic and language difficulties are common and can worsen behavioral symptoms when left unaddressed.
- Substance use disorders: Risk increases in adolescents with untreated ODD, particularly those who also have ADHD or conduct disorder.
Treatment for Oppositional Defiant Disorder
ODD is treatable. A comprehensive plan involving the child, family, school, and mental health providers produces the best outcomes. Medication is not recommended as first-line treatment for ODD itself, but may be prescribed for comorbid conditions.
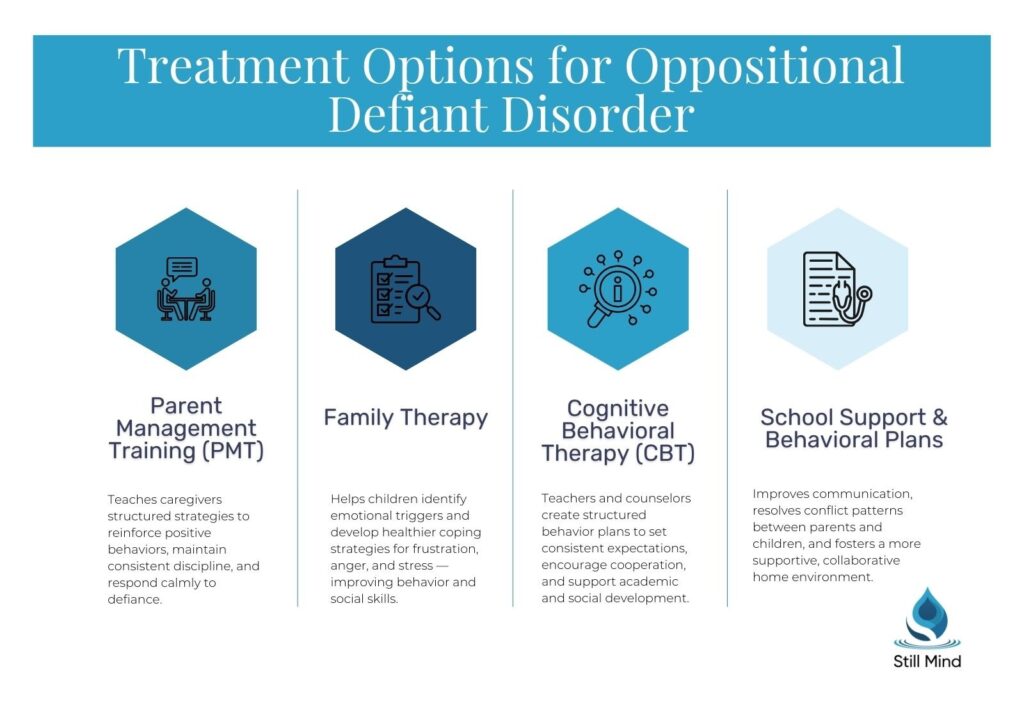
1. Parent Management Training (PMT)
Parent management training is consistently the most effective intervention, particularly for younger children. A behavioral health specialist teaches parents evidence-based strategies for setting limits, reinforcing positive behavior, and responding consistently to defiance.
2. Cognitive Behavioral Therapy (CBT)
Cognitive behavioral therapy helps children identify distorted thinking patterns that fuel defiant behavior. It builds skills in problem-solving, impulse control, and anger management, and is especially effective in school-age children and adolescents.
3. Family Therapy
Family therapy addresses communication breakdowns and conflict cycles that maintain ODD behaviors. It teaches healthier interaction patterns and helps siblings and other caregivers understand and respond to the child’s behavior consistently.
4. School-Based Interventions
Coordination between treatment providers and educators is critical. Children with ODD may qualify for accommodations under Section 504 or the Individuals with Disabilities Education Act (IDEA), depending on the degree of academic impairment.
5. Anger Management and Social Skills Training
Structured programs in anger management techniques and social skills training help children learn to navigate frustration, resolve conflicts, and build peer relationships without resorting to defiance or retaliation.
6. Medication
No medications are specifically approved to treat ODD. However, stimulants or non-stimulant ADHD medications can reduce oppositional symptoms in children with comorbid ADHD. Antidepressants and mood stabilizers may help when anxiety or depression is also present.
Can ODD Be Prevented?
ODD cannot always be prevented, but early intervention can significantly reduce its severity and long-term impact. Recognizing risk factors early and acting on them gives families the best chance of better outcomes.
Strategies that support prevention include:
- Providing a warm, structured, and predictable home environment
- Using consistent, non-punitive discipline strategies from early childhood
- Accessing early childhood programs like Head Start for high-risk families
- Addressing parental mental health, including untreated ADHD or mood disorders
- Treating anxiety and learning differences in children before they compound behavioral difficulties
When to Seek Help for ODD
Parents often second-guess whether their child’s behavior crosses the threshold from normal into clinical. A few clear indicators that a professional evaluation is warranted include:
- Defiant behavior occurs nearly every day and has lasted more than six months
- The behavior causes significant problems at home, school, or with peers
- The child shows signs of vindictiveness, deliberate provocation, or emotional cruelty
- Other adults (teachers, extended family) are expressing concern about the behavior
- You suspect ADHD, anxiety, or another condition may be co-occurring
If you are concerned about your child’s behavioral and emotional health, our team at Still Mind Florida can help. We provide comprehensive mental health evaluations and evidence-based residential treatment for adolescents and adults navigating complex behavioral conditions. Contact our admissions team to learn more.
Frequently Asked Questions
What is the main cause of oppositional defiant disorder?
No single cause has been identified. ODD results from a combination of genetic predisposition, neurobiological differences in emotional regulation, and environmental factors such as inconsistent parenting, family stress, and early trauma. Children with a parent who has ADHD or a behavioral disorder carry a higher biological risk.
What are the three categories of ODD symptoms?
The DSM-5 groups ODD symptoms into three categories: angry or irritable mood (frequent temper loss, touchiness, resentment), argumentative or defiant behavior (refusing rules, arguing, blaming others), and vindictiveness (spiteful or retaliatory behavior occurring at least twice in six months). At least four symptoms across any category must be present for diagnosis.
Is ODD different from conduct disorder?
Yes. ODD involves defiance, anger, and vindictiveness. Conduct disorder involves more serious violations, including physical aggression, cruelty to people or animals, theft, and destruction of property. About 30% of children with ODD develop conduct disorder if symptoms go untreated.
Can ODD occur in adults?
Yes. ODD can persist into or first emerge in adulthood, though it is less commonly diagnosed in that population. Adults with ODD may display chronic conflict with authority figures at work or in relationships. It is frequently misidentified as a personality disorder and often co-occurs with depression or substance use.
How long does ODD treatment take?
There is no fixed timeline. Many children show meaningful improvement within several months of consistent parent management training and therapy. Severity, the presence of comorbid conditions, and family engagement all affect duration. Early intervention consistently produces better and faster outcomes than delayed treatment.
Is ODD linked to autism or ADHD?
Both connections exist. ADHD is the most common ODD comorbidity, present in a large percentage of diagnosed children. Autism and ODD can appear similar due to overlapping behavioral features, and some researchers believe defiant behavior in autistic children may reflect a response to environmental demands rather than a separate condition. A comprehensive evaluation is essential to differentiate accurately.
References
- American Academy of Family Physicians. (2016). Common questions about oppositional defiant disorder. American Family Physician, 93(7), 586-595.
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). American Psychiatric Publishing.
- Cleveland Clinic. (2022). Oppositional defiant disorder (ODD). Cleveland Clinic.
- Hawes, D. J., Gardner, F., Dadds, M. R., Frick, P. J., Kimonis, E. R., Burke, J. D., and Fairchild, G. (2023). Oppositional defiant disorder. Nature Reviews Disease Primers, 9(1), 31.
- Johns Hopkins Medicine. (2024). Oppositional defiant disorder. Johns Hopkins Medicine.
- Mayo Clinic. (2023). Oppositional defiant disorder (ODD): Symptoms and causes. Mayo Clinic.
- National Institute of Mental Health. (2023). Child and adolescent mental health. U.S. Department of Health and Human Services.
- Oppositional defiant disorder. (2024). In StatPearls. National Center for Biotechnology Information. https://www.ncbi.nlm.nih.gov/books/NBK557443/