




Anhedonia is the inability to feel pleasure or interest in activities that once brought enjoyment. It is not sadness, it is emotional flatness, a dulling of the reward system that makes food, hobbies, relationships, and everyday experiences feel empty or meaningless.
Anhedonia is one of the two core diagnostic symptoms of major depressive disorder, but it also appears in bipolar disorder, schizophrenia, PTSD, and other conditions. This article explains what anhedonia is, what causes it, how to recognize it, and how it is treated.
Key Highlights
- Anhedonia is one of two core symptoms required for a diagnosis of major depressive disorder under DSM-5, alongside depressed mood.
- It is primarily driven by disruption in the brain’s dopamine reward pathway, particularly reduced activity in the ventral striatum and nucleus accumbens.
- Research published in PMC found that vitamin D-deficient patients scored significantly higher on anhedonia symptom factors than those with sufficient vitamin D levels.
- Anhedonia is associated with higher suicidal ideation independent of overall depression severity, making early identification clinically critical.
- Standard SSRIs may not adequately treat anhedonia; dopamine-targeting medications, behavioral activation, and TMS show stronger evidence for directly addressing reward system dysfunction.
What Does Anhedonia Mean?
The word anhedonia comes from the Greek “an” (without) and “hedone” (pleasure). It was first coined by French psychologist Théodule-Armand Ribot in 1896 to describe the complete loss of pleasure in melancholia. Today the term applies more broadly to any significant reduction in the capacity to experience or anticipate pleasure.
Anhedonia is not a standalone diagnosis. It is a symptom of an underlying condition. However, researchers increasingly recognize it as a partially independent phenomenon that deserves targeted clinical attention, not just treatment of the parent disorder. A person may have significant anhedonia with mild overall depression, or experience anhedonia as the primary burden of their illness.
Is Anhedonia a Disorder or a Symptom?
Anhedonia is classified as a symptom, not an independent disorder in the DSM-5. It does not have its own diagnostic code. What gives anhedonia clinical weight is its role as a mandatory criterion for diagnosing major depressive disorder. Under DSM-5, a person must exhibit either persistent depressed mood or anhedonia as the foundation of an MDD diagnosis all other criteria build on one of these two.
Despite this classification, the research community is increasingly treating anhedonia as a distinct clinical target. Studies show it can persist after other depressive symptoms remit, predict poorer treatment outcomes, and carry its own independent risk for suicidality. In that sense, it behaves more like a condition than a simple symptom.
Types of Anhedonia
Anhedonia is commonly divided into two subtypes based on which domain of pleasure is affected.
Social Anhedonia
Social anhedonia is a reduced or absent desire for human connection and social interaction. A person may stop reaching out to friends, withdraw from family events, or feel nothing when spending time with people they previously enjoyed. This differs from social anxiety, which involves fear of judgment. In social anhedonia, there is no fear; there is simply no pull toward connection at all.
Social anhedonia is particularly prominent in schizophrenia spectrum disorders and is associated with poorer long-term social functioning. Research consistently shows that males score higher on social anhedonia measures than females, and this difference is stable from adolescence into adulthood.
Physical Anhedonia
Physical anhedonia refers to the reduced capacity to experience pleasure from sensory experiences: food, music, touch, sex, physical activity, or the natural environment. Things that once had a distinct pleasurable quality become neutral or flat. Meals feel mechanical. Music sounds like noise. Exercise feels like an obligation rather than a release.
Physical anhedonia is frequently reported in major depressive disorder, bipolar disorder, and substance use disorders, especially during or after periods of heavy use.
Anhedonia Symptoms
Anhedonia does not always look like obvious sadness. Many people with anhedonia describe feeling emotionally flat or numb rather than visibly upset. This can make it harder to recognize, both for the person experiencing it and for those around them.
Common signs of anhedonia include:
- Loss of interest in previously enjoyed hobbies: Activities like reading, gaming, cooking, or sports that once occupied hours no longer hold any appeal or motivation
- Reduced enjoyment from food: Eating feels like a mechanical necessity rather than a pleasurable experience; taste may feel diminished
- Emotional detachment from relationships: Feeling little or nothing when spending time with people you care about, or no longer wanting to initiate contact
- Decreased motivation: Difficulty starting or sustaining any activity without an external push, as nothing feels rewarding enough to justify the effort
- Reduced or absent sexual interest: Loss of libido or the absence of pleasure during sexual activity
- Flat emotional responses: Watching events unfold, including things that should be exciting or moving, without any accompanying emotional response
- Difficulty anticipating pleasure: Unable to look forward to events or experiences that would previously have generated excitement or anticipation
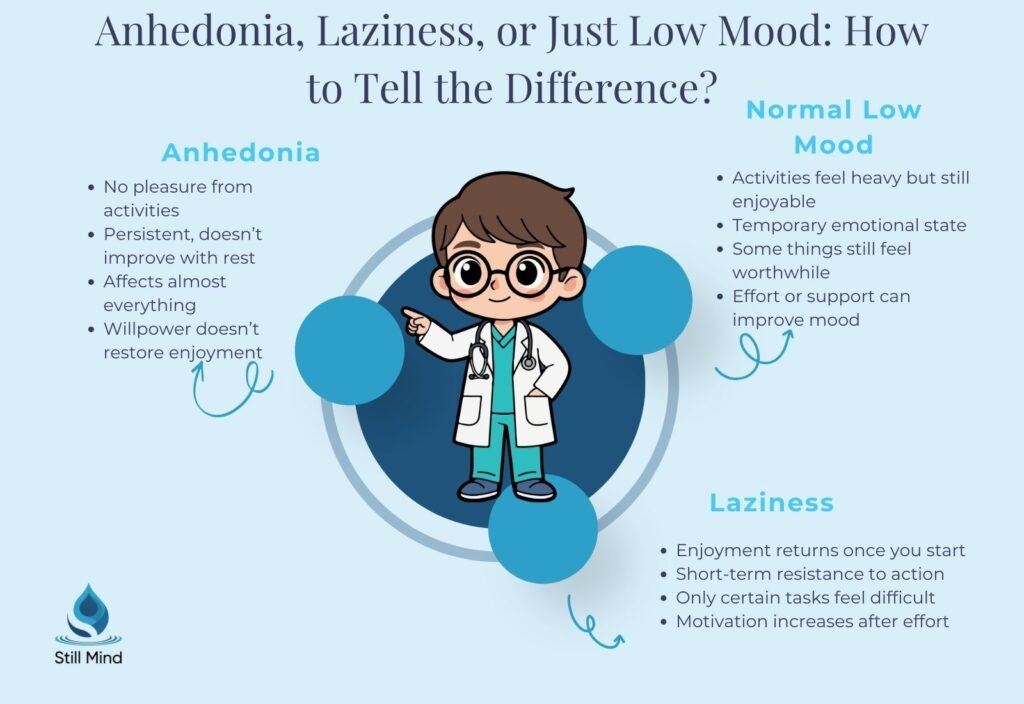
Anhedonia frequently co-occurs with depression, but the relationship is not one-to-one. A person can experience anhedonia without a deeply sad mood, and can have depression without prominent anhedonia. Recognizing the difference matters because treatment approaches can differ.
What Causes Anhedonia?
Anhedonia results from disruption in the brain’s reward processing system, particularly the circuits involving dopamine. The exact mechanisms vary, but several biological and environmental factors are consistently implicated.
Dopamine and the Reward System
Dopamine is the primary neurotransmitter governing the brain’s reward pathway. When the brain anticipates or receives a reward, it signals the ventral tegmental area to release dopamine into the nucleus accumbens the region often called the brain’s “pleasure center.” Reduced dopamine activity in this circuit is the most well-established neurobiological mechanism of anhedonia.
Disruption can occur at multiple points: the brain may not produce enough dopamine, may lack sufficient dopamine receptors, or may not respond normally to dopamine that is released. Chronic stress, substance use, and certain medications can all degrade this system over time. Understanding how anhedonia overlaps with hyperfixation and motivation-related patterns can help clarify why the reward system behaves inconsistently in these conditions.
Inflammation
Elevated inflammatory markers, particularly C-reactive protein (CRP) and certain cytokines, are associated with reduced connectivity between the ventral striatum and the prefrontal cortex. This disrupted connectivity maps directly onto the impaired reward anticipation and motivation that characterize anhedonia. Inflammatory conditions, including autoimmune disorders and chronic illness, can trigger or worsen anhedonia through this mechanism.
Underlying Mental Health Conditions
Anhedonia appears across a wide range of psychiatric diagnoses. Major depressive disorder is the most common context, but anhedonia is also prominent in bipolar disorder, schizophrenia spectrum disorders, PTSD, and certain personality disorders. People with bipolar disorder and schizophrenia frequently experience anhedonia as one of the most impairing features of their illness.
Chronic Stress
Sustained psychological stress elevates cortisol, which interferes with dopamine signaling. Over time, chronic stress suppresses the brain’s natural reward response, making ordinary pleasures feel progressively less rewarding. This is one of the pathways through which prolonged burnout, trauma exposure, and emotional exhaustion can develop into clinical anhedonia.
Substance Use
Repeated substance use floods the dopamine system with artificially high levels, which the brain compensates for by downregulating dopamine receptors. When the substance is removed, the depleted dopamine system struggles to register natural rewards. This is why anhedonia is common during withdrawal and early recovery from addiction.
What Deficiency Causes Anhedonia?
Vitamin D deficiency is the most clinically studied nutritional factor linked to anhedonia. Research published in PMC found that patients hospitalized with a depressive episode who had vitamin D deficiency scored significantly higher on anhedonia symptom factors compared to those with sufficient vitamin D levels. The connection is neurobiological: vitamin D plays a protective role in dopaminergic neurons and is involved in the regulation of dopamine transporter expression in the nucleus accumbens.
Other nutritional factors that may contribute include deficiencies in B vitamins (particularly B6, B9, and B12), iron, and magnesium, all of which are involved in dopamine synthesis and neurotransmitter function. Thyroid dysfunction (hypothyroidism) can also produce anhedonia-like symptoms by broadly suppressing metabolic and neurological function.
Ruling out these physical causes is a standard part of the clinical evaluation process and does not require a formal psychiatric assessment to begin.
Anhedonia and Depression: How They Differ
| Feature | Anhedonia | Major Depression |
|---|---|---|
| Core experience | Absence of pleasure and interest | Persistent sadness, hopelessness, and low mood |
| Emotional tone | Flat, empty, numb | Sad, tearful, hopeless, or irritable |
| Can occur independently | Yes, without depression | Yes, without prominent anhedonia |
| Neurobiology | Primarily dopamine and reward circuitry | Serotonin, norepinephrine, dopamine, HPA axis |
| Response to SSRIs | Limited; may worsen in some cases | Often improves with standard antidepressant treatment |
| DSM-5 status | Core symptom, not an independent diagnosis | Standalone diagnosis with formal criteria |
How to Test for Anhedonia
There is no blood test or imaging scan that directly measures anhedonia. Assessment relies on clinical evaluation and validated self-report tools. The most widely used instrument is the Snaith-Hamilton Pleasure Scale (SHAPS), a brief 14-item questionnaire that asks about pleasure across multiple life domains including food, social activities, sensory experiences, and hobbies.
Other assessment tools include the Chapman Physical Anhedonia Scale (CPAS), the Positive and Negative Affect Schedule (PANAS), and the Fawcett-Clark Pleasure Scale (FCPS). These instruments help clinicians distinguish between anhedonia and general depression severity, which matters for treatment planning.
A comprehensive evaluation also includes a physical exam, blood tests to rule out vitamin D deficiency and thyroid dysfunction, a full psychiatric history, and questions about substance use. Only a licensed clinician can formally evaluate and diagnose the underlying condition causing anhedonia.
Is Anhedonia Permanent?
Anhedonia is not permanent in most cases, but it does not resolve on its own without treating the underlying cause. With appropriate treatment, the majority of people experience meaningful improvement in their capacity for pleasure and interest. That said, anhedonia can be stubborn, particularly when it is caused by chronic depression, schizophrenia, or long-term substance use that has caused lasting changes to the dopamine system.
Recovery is typically gradual. People often notice small improvements first, a moment of genuine interest in something, or a meal that actually tasted good, before larger changes become consistent. Anhedonia may recur if the underlying condition is not well managed, which is why maintenance treatment and follow-up care matter after initial improvement.
Best Treatments for Anhedonia
There is no single approved treatment specifically for anhedonia. Treatment is directed at the underlying condition and, when possible, at the reward system dysfunction itself. The most effective approaches combine behavioral and pharmacological strategies.
Behavioral Activation Therapy
Behavioral activation is among the most evidence-supported treatments specifically for anhedonia. Unlike standard CBT, which focuses on changing thought patterns, behavioral activation works by systematically re-engaging a person with activities that have the potential to generate reward. The approach is graded and deliberate: small, manageable activities come first, building momentum and slowly restoring the brain’s reward responsiveness through repeated positive exposure.
Research shows behavioral activation can lower depression symptoms long-term and is particularly effective when standard CBT has limited effect on the loss of pleasure itself.
Cognitive Behavioral Therapy (CBT)
CBT helps address the negative thought patterns, avoidance behaviors, and cognitive distortions that reinforce anhedonia. Cognitive behavioral therapy is often combined with behavioral activation for the most comprehensive approach, targeting both the thought patterns and the behavioral withdrawal that sustain anhedonia over time.
Medication
Standard SSRIs have limited and inconsistent effects on anhedonia and may worsen emotional flatness in some individuals. Medications that more directly target the dopamine system tend to show better results. These include bupropion (which affects both dopamine and norepinephrine), stimulant augmentation with methylphenidate, agomelatine, and vortioxetine. Ketamine and its derivatives have shown rapid anti-anhedonic effects in treatment-resistant cases, with one study reporting symptom relief within 40 minutes of infusion.
For those considering ketamine, understanding the current evidence and risks is important. Our article on ketamine therapy for depression examines what the research supports and what to consider before pursuing this option.
Transcranial Magnetic Stimulation (TMS)
TMS delivers targeted magnetic pulses to the dorsolateral prefrontal cortex, stimulating the reward-related circuits that are underactive in anhedonia. A systematic review and meta-analysis found that TMS interventions produced significant improvements in anhedonia symptoms, with medium-to-large effect sizes in both schizophrenia and depression studies. TMS is particularly relevant for individuals who have not responded to medication.
Exercise and Lifestyle
Aerobic exercise and strength training generate dopamine and adrenaline, providing both immediate mood effects and long-term benefits to the reward system. Regular physical activity is one of the few self-directed interventions with solid evidence for reducing anhedonia symptoms, particularly in people recovering from substance use disorders. Correcting nutritional deficiencies (vitamin D, B vitamins, and iron) should also be addressed as part of a comprehensive recovery plan.
Frequently Asked Questions
What is the best treatment for anhedonia?
There is no single best treatment, as anhedonia requires targeting both the underlying condition and the reward system dysfunction directly. The most evidence-supported approaches are behavioral activation therapy, CBT combined with behavioral activation, and dopamine-targeting medications such as bupropion. For treatment-resistant cases, TMS and ketamine show strong and often rapid results. Regular aerobic exercise and correction of vitamin D or other nutritional deficiencies are important adjuncts. A psychiatrist or clinical team should guide the treatment plan based on the specific underlying diagnosis.
What are the main causes of anhedonia?
The primary cause is disruption in the brain’s dopamine-driven reward system, particularly reduced activity in the ventral striatum and nucleus accumbens. Contributing factors include major depression, bipolar disorder, schizophrenia, PTSD, chronic stress, substance use disorder, inflammation, and nutritional deficiencies such as vitamin D. In some cases, certain antidepressants (especially SSRIs) can cause or worsen emotional flatness that resembles anhedonia.
How do you test for anhedonia?
Assessment uses validated self-report scales, particularly the Snaith-Hamilton Pleasure Scale (SHAPS), combined with a clinical interview. A clinician will also order blood tests to rule out vitamin D deficiency and thyroid dysfunction, and take a full psychiatric and substance use history. Anhedonia does not have a standalone diagnostic code the evaluation focuses on identifying the underlying condition responsible for the symptom and measuring its severity across physical and social domains.
What deficiency causes anhedonia?
Vitamin D deficiency is the most studied nutritional factor linked to anhedonia, with research showing significantly higher anhedonia scores in people with vitamin D levels below 50 nmol/l compared to those with sufficient levels. Vitamin D supports dopaminergic neurons and regulates dopamine transporter expression in reward-related brain areas. B vitamin deficiencies (B6, B9, B12), iron deficiency, and magnesium insufficiency may also impair dopamine synthesis and worsen symptoms. Thyroid dysfunction should be ruled out as well.
Is anhedonia the same as being depressed?
No. Anhedonia is a symptom that can occur within depression, but the two are not identical. Depression involves a broader cluster of symptoms, including sadness, guilt, fatigue, and sleep changes. Anhedonia specifically refers to the inability to feel pleasure or interest. A person can have significant anhedonia with little sadness, or can be deeply depressed without the reward system impairment that defines anhedonia. This distinction matters because treatment approaches, particularly around medication selection, differ depending on which symptom is most prominent.
Bottom Line
Anhedonia is a serious, treatable symptom that signals a meaningful disruption in the brain’s reward system. It rarely resolves without clinical support, but with the right combination of therapy, medication, and lifestyle change, most people experience genuine recovery of their capacity for pleasure.
If you or someone you care about is experiencing a persistent loss of interest and pleasure in life, Still Mind Florida offers residential mental health treatment that addresses depression, anhedonia, and co-occurring conditions through individualized, evidence-based care. Reach out through our admissions page to learn more about how we can help.
References
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). American Psychiatric Publishing.
- Penninx, B. W. J. H., Milaneschi, Y., Lamers, F., & Vogelzangs, N. (2013). Understanding the somatic consequences of depression: Biological mechanisms and the role of depression symptom profile. BMC Medicine, 11, 129.
- Buckner, J. D., et al. (2023). Anhedonia and depressive disorders. PMC Translational Psychiatry.
- Gruenberg, A. M., Goldstein, R. D., & Pincus, H. A. (2005). Classification of depression: Research and diagnostic criteria. Biology of Depression, 1–12.
- Shafer, A. B. (2006). Meta-analysis of the factor structures of four depression questionnaires: Beck, CES-D, Hamilton, and Zung. Journal of Clinical Psychology, 62(1), 123–146.
- Grunebaum, M. F., Galfalvy, H. C., Mortenson, L. Y., Burke, A. K., Oquendo, M. A., & Mann, J. J. (2017). Anhedonia and suicidal ideation in bipolar disorder. Psychiatry Research, 252, 195–200.
- Spijker, J., et al. (2015). Vitamin D deficiency and depressive symptomatology in psychiatric patients hospitalized with a current depressive episode. PLOS ONE.
- Gupta, S. K., Bhaskaran, L., & Dharmalingam, M. (2022). Is vitamin D important in anxiety or depression? What is the truth? PMC.
- Cleveland Clinic. (2023). Anhedonia: What it is, causes, symptoms and treatment.
- National Center for Biotechnology Information. (2023). Major depressive disorder. StatPearls. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK559078/