




Anhedonia is the loss of the ability to feel pleasure, and it is a recognized clinical symptom rather than a phase that passes on its own.
It most commonly accompanies major depression, but it can arise during substance use recovery, after trauma, and across a range of other conditions. With proper treatment, most people recover the capacity to feel reward and connection. If life has started to feel flat, colorless, or empty without an obvious reason, anhedonia may be what you are experiencing.
Key Takeaways
- Anhedonia is the clinically defined inability to experience pleasure from activities, relationships, or experiences that once brought enjoyment.
- The DSM-5 identifies anhedonia as one of two core diagnostic criteria for major depressive disorder, alongside persistently depressed mood.
- Three primary types are documented in research: physical anhedonia, social anhedonia, and anticipatory anhedonia.
- The core neurological mechanism is dopaminergic dysfunction in the reward circuit, including the ventral striatum, nucleus accumbens, and prefrontal cortex.
- With treatment, depression-related anhedonia typically improves within 6 to 12 weeks; substance-related anhedonia requires several months of sobriety and targeted support.
- According to a 2023 PMC review, SSRIs show limited and sometimes counterproductive results for anhedonia; dopamine-targeting medications, behavioral activation, CBT, and TMS have stronger clinical evidence.
What Anhedonia Means
Anhedonia specifically describes a deficit in the brain’s reward-processing system, not general sadness or emotional pain.
The Clinical Definition
What the DSM-5 and current psychiatric research establish about anhedonia meaning:
- The DSM-5 defines anhedonia as “lack of enjoyment from, engagement in, or energy for life’s experiences; deficits in the capacity to feel pleasure and take interest in things” (American Psychiatric Association, 2013).
- It is classified as a facet of the broad personality trait domain of detachment, reflecting a fundamental withdrawal from positive emotional experience at a neurobiological level.
- A 2024 systematic review in CNS Drugs categorizes anhedonia as an independent transdiagnostic domain that independently predicts poorer outcomes, reduced quality of life, and higher relapse rates across multiple psychiatric conditions.
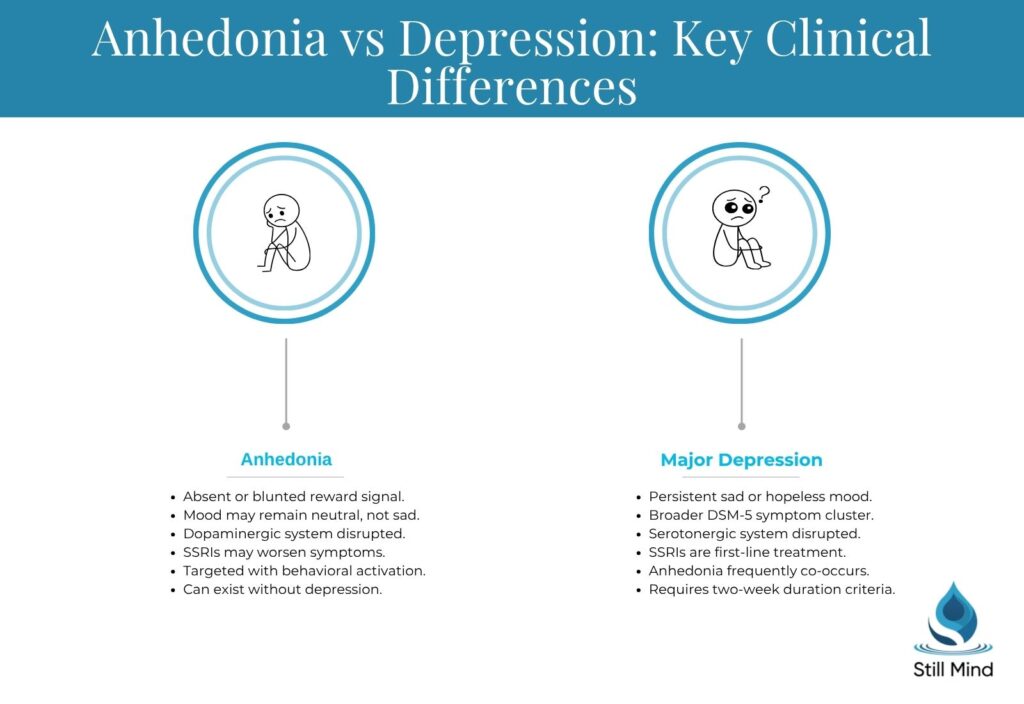
Anhedonia vs Depression: Where They Diverge
Anhedonia and major depressive disorder share significant clinical overlap, but they are not identical and do not always respond to the same treatments.
Key distinctions between anhedonia vs depression:
- Depression encompasses a broad symptom cluster including persistent sadness, worthlessness, cognitive slowing, and somatic changes; anhedonia can occur without most of these.
- A person can experience clinically significant anhedonia while reporting a neutral rather than depressed mood, particularly in schizophrenia, post-acute withdrawal syndrome (PAWS), or Parkinson’s disease.
- A 2023 PMC review concludes that anhedonia is at least partially independent from depression, and that serotonin-focused treatments frequently fail to address its underlying dopaminergic deficit.
Anhedonia vs Apathy: A Key Distinction
Apathy and anhedonia are frequently confused in clinical practice, but they originate from different neural systems and require different interventions.
What separates them clinically:
- Anhedonia is a reward-processing deficit: the brain’s dopaminergic system fails to generate or register pleasure, even when external rewards are present.
- Apathy is a motivational deficit: reduced initiation and persistence of goal-directed behavior, which can exist even when pleasure capacity remains largely intact.
- Identifying which is primary matters for treatment selection, because underlying emotional dysregulation can drive both conditions through separate neurological pathways.
The Three Types of Anhedonia
Anhedonia is not a single uniform experience; it divides into distinct subtypes that each disrupt different domains of reward processing.
Physical Anhedonia
What physical anhedonia involves:
- Reduced or absent pleasure from sensory experiences such as food, touch, warmth, physical activity, and music, even when sensory perception itself remains intact.
- The person may continue eating, exercising, or engaging in activities but reports a blunted or completely absent internal sense of enjoyment or reward.
- Musical anhedonia is a recognized and measurable variant describing a specific loss of emotional response to music, independent of hearing ability or musical familiarity.
Social Anhedonia
What social anhedonia involves:
- Reduced or absent pleasure from social interactions, conversations, and interpersonal connection, which gradually produces withdrawal and isolation.
- Social anhedonia is a documented risk factor for schizophrenia-spectrum disorders and is associated with diminished relationship quality and progressive social disengagement over time.
- Research synthesis notes that males score consistently higher than females on validated social anhedonia measures, a difference that remains stable from adolescence through adulthood.
Anticipatory Anhedonia
What anticipatory anhedonia involves:
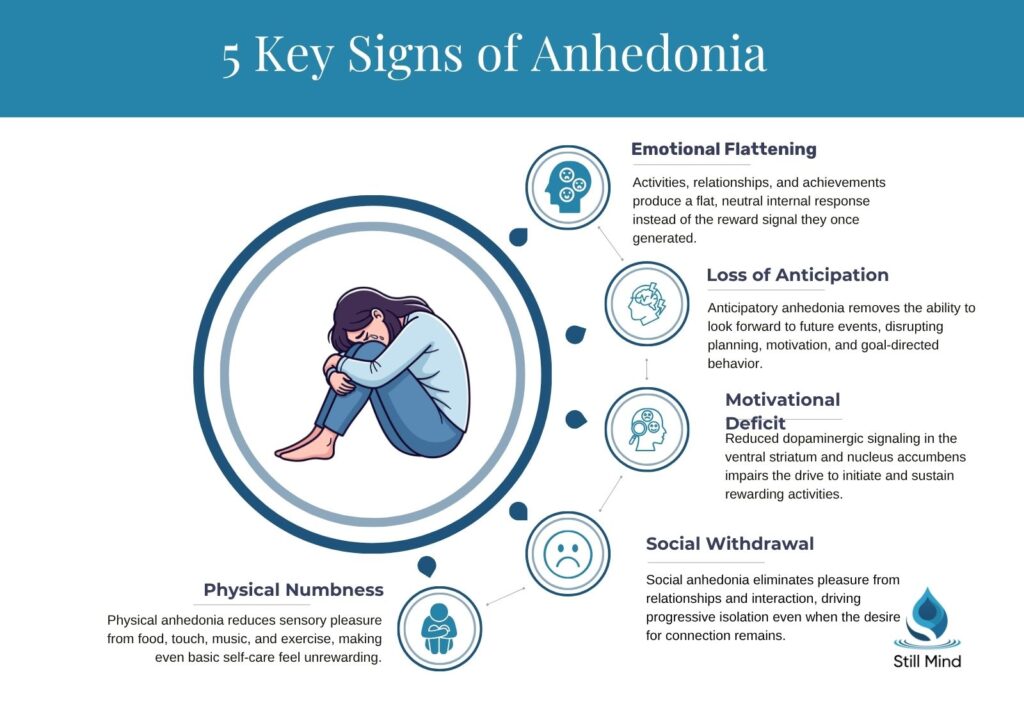
- Loss of the ability to look forward to future events, plans, or experiences, disrupting motivation and goal-directed behavior even when in-the-moment enjoyment may still partially occur.
- It is distinguished from consummatory anhedonia, which describes the inability to feel pleasure during an experience rather than before it.
- Anticipatory anhedonia is particularly prominent in depression and post-traumatic conditions, where patterns of rumination about negative futures compound the motivational deficit.
What Anhedonia Feels Like: Core Symptoms
The experience of anhedonia extends beyond not enjoying things and affects emotional, behavioral, and physical functioning across daily life.
Emotional Flattening
Emotional changes that mark anhedonic states:
- Activities, relationships, and accomplishments that previously generated excitement, pride, or warmth now produce a flat, neutral, or numb internal response.
- The dominant experience is absence rather than pain: an inability to feel reward rather than an intensely negative emotional state.
- This distinguishes anhedonia from grief or clinical sadness, where emotional pain is present and intense, even if difficult to endure.
Social and Behavioral Withdrawal
Behavioral patterns commonly associated with anhedonia:
- Withdrawal from hobbies, social settings, and close relationships, driven not by fear or conflict but by the absence of anticipated reward.
- Reduced motivation to pursue previously meaningful goals, maintain fulfilling routines, or initiate contact with others.
- The withdrawal intensifies the problem: decreased positive environmental stimulation further suppresses an already underactive reward circuit, creating a self-reinforcing anhedonic cycle.
Physical and Motivational Symptoms
Physical dimensions that accompany the emotional deficit:
- Fatigue, low energy, disrupted sleep, and changes in appetite frequently accompany anhedonia, particularly when linked to major depressive disorder or post-acute withdrawal.
- Diminished interest in previously enjoyed foods reflects the sensory dimension of reward-circuit suppression, not simply reduced hunger.
- When anhedonia co-occurs with burnout, physical exhaustion and dopaminergic downregulation reinforce each other and both require targeted clinical attention.
What Causes Anhedonia
Anhedonia develops when the brain’s reward-processing system is disrupted, whether neurochemically, structurally, or through chronic exposure to stress or trauma.
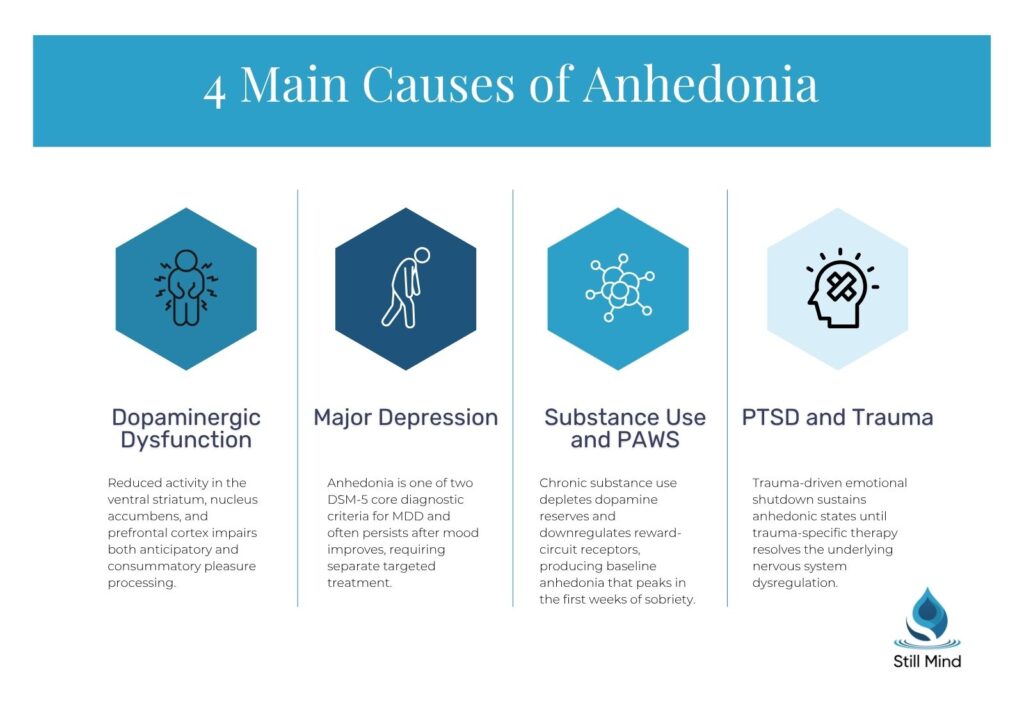
Dopaminergic Reward Circuit Disruption
The core neurological mechanism underlying anhedonia causes:
- Functional imaging studies identify the ventral striatum, nucleus accumbens, and prefrontal cortex as key nodes in the reward circuit implicated in anhedonia, according to a 2024 CNS Drugs review.
- Reduced dopaminergic signaling through these pathways impairs both anticipatory pleasure and consummatory enjoyment, producing the characteristic flatness of anhedonic experience.
- Glutamatergic and serotonergic alterations also contribute to the deficit, which explains why serotonin-targeted treatments produce limited and inconsistent improvement.
Underlying Mental Health and Medical Conditions
Conditions that commonly produce anhedonia as a core feature:
- Major depressive disorder, where anhedonia is one of two DSM-5 core diagnostic criteria alongside persistently depressed mood.
- Schizophrenia, where negative symptom clusters heavily involve reward-circuit dysfunction, persistent social anhedonia, and motivational deficits.
- Bipolar disorder, PTSD, eating disorders, anxiety disorders, Parkinson’s disease, Cushing’s disease, and traumatic brain injury are all documented clinical causes.
Substance Use and Post-Acute Withdrawal
How addiction-related neurological damage produces anhedonia:
- Chronic substance use depletes dopamine reserves and downregulates reward-circuit receptors, producing a baseline anhedonic state that persists into early sobriety.
- In post-acute withdrawal syndrome following opioid, methamphetamine, or alcohol cessation, anhedonia typically peaks in the first two to four weeks of abstinence.
- Treating anhedonia as a recognized clinical feature of addiction recovery supports treatment engagement and reduces the relapse risk that comes from an inability to feel pleasure in sobriety.
How Long Does Anhedonia Last
How long anhedonia lasts depends on the underlying cause, the severity of reward-circuit disruption, and whether treatment is applied consistently.
Depression-Related Anhedonia
Duration timeline for anhedonia linked to major depressive disorder:
- Without treatment, depression-related anhedonia persists for weeks to months; in untreated moderate-to-severe MDD, cases can extend beyond a year without intervention.
- With therapy, targeted medication, and lifestyle changes, most people notice meaningful improvement within 6 to 12 weeks, according to clinical guidance from Cleveland Clinic.
- Pleasure restoration may lag behind general mood improvement, with anhedonia sometimes the last symptom to fully resolve in otherwise treatment-responsive patients.
Anhedonia in Addiction Recovery
How long substance-related anhedonia lasts during PAWS:
- Anhedonia in early sobriety typically peaks in the first few weeks of abstinence and then gradually improves over three to twelve months as the dopaminergic system heals.
- Duration varies significantly based on substance type, duration of use, and whether co-occurring depression or PTSD receives simultaneous treatment.
- Aerobic exercise is a clinically supported behavioral intervention during recovery, generating endogenous dopamine and accelerating reward-circuit rehabilitation without requiring adjunctive medication.
PTSD and Trauma-Related Anhedonia
How long trauma-driven anhedonia can persist:
- When anhedonia is sustained by unresolved trauma or PTSD, it typically does not resolve until trauma processing occurs through specialized, targeted therapy.
- EMDR therapy and trauma-focused CBT are evidence-supported approaches for breaking the cycle of emotional shutdown that maintains trauma-linked anhedonic states.
- Without trauma-specific treatment, PTSD-related anhedonia can persist for years; with appropriate care, consistent and measurable improvement is the expected clinical outcome.
Is Anhedonia Permanent
Anhedonia is rarely permanent when appropriate treatment is applied, as the brain’s reward system retains significant neuroplastic capacity for recovery in most clinical presentations.
The Evidence on Prognosis
What research shows about long-term recovery from anhedonia:
- No evidence supports irreversibility in the absence of structural brain damage; neuroplasticity allows reward circuits to normalize with sustained and targeted intervention.
- Most people with treatment-responsive depression, substance use disorders, or PTSD regain functional pleasure capacity, particularly with dopamine-targeted therapy, behavioral activation, or neuromodulation.
- A 2024 CNS Drugs review reports that maintaining hedonic improvements is both feasible and beneficial, with multiple long-term analyses supporting sustained remission of anhedonic symptoms.
Warning Signs Requiring Immediate Help
When anhedonia indicates a clinical emergency:
- Anhedonia accompanied by suicidal ideation, self-harm thoughts, or a complete inability to maintain basic self-care requires immediate clinical evaluation without delay.
- Higher anhedonia levels are independently associated with elevated suicidal ideation in both cross-sectional and longitudinal research, operating as a risk factor separate from overall depression severity (PMC, 2023).
- Inability to eat, sleep, or maintain daily routines for more than two weeks without any improvement is a clear indicator that professional evaluation should not be postponed.
How Anhedonia Is Treated
Anhedonia responds best to treatments that directly target reward-circuit dysfunction rather than approaches designed primarily for general mood symptoms.
Behavioral Activation and CBT
First-line psychotherapeutic approaches for how to fix anhedonia:
- Behavioral activation (BA) systematically increases exposure to rewarding activities to reactivate suppressed dopaminergic pathways, and is among the most evidence-supported behavioral interventions for anhedonia.
- Cognitive behavioral therapy targets avoidance-reinforcing beliefs that sustain anhedonic withdrawal and builds practical skills for re-engagement with previously meaningful activities.
- CBT combined with BA produces stronger outcomes than either intervention alone, according to PMC research and APA-endorsed clinical guidelines for depression and anhedonia treatment.
Positive Affect Treatment
A specialized intervention targeting reward-system retraining:
- Positive Affect Treatment (PAT) is a structured therapy built to directly rebuild the brain’s ability to anticipate and experience positive emotion through targeted reward-pathway retraining.
- It incorporates savoring techniques, gratitude practices, and positive emotion amplification exercises that restore hedonic capacity rather than simply reducing negative symptoms.
- PAT is particularly effective for anticipatory anhedonia, directly addressing the inability to generate forward-looking positive affect that makes motivation and goal-setting feel inaccessible.
Dopamine-Targeting Medications
Pharmacological options better matched to anhedonia’s neurochemistry than standard antidepressants:
- SSRIs produce a pro-anhedonic effect in some patients by broadly blunting emotional responsiveness; dopamine-targeting medications are more appropriate as frontline options for anhedonic presentations.
- Bupropion, agomelatine, and vortioxetine carry stronger and more consistent evidence for improving anhedonic symptoms than serotonin-focused antidepressants, according to a 2023 PMC review.
- Dopaminergic stimulants such as methylphenidate may be used adjunctively, particularly when motivational anhedonia is the dominant clinical presentation.
Ketamine, TMS, and Neuromodulation
Interventional options for treatment-resistant or severe anhedonia:
- Ketamine produces rapid anti-anhedonic effects: a 2024 meta-analysis found significant symptom improvement in both unipolar and bipolar depression, with some patients reporting relief within 40 minutes of infusion.
- Repetitive TMS and transcranial direct current stimulation (tDCS) target reward-circuit hypoactivity directly; a meta-analysis reported Hedges’ g of 0.443 in sham-controlled depression trials and 0.665 in schizophrenia studies.
- Somatic therapy provides a body-based complement to pharmacological and behavioral treatment, supporting nervous system regulation that underlies reward-circuit recovery.
Frequently Asked Questions About Anhedonia
How do you fix anhedonia?
Fixing anhedonia requires identifying and treating the underlying cause first. Behavioral activation and CBT are effective first-line approaches. Dopamine-targeting medications such as bupropion, agomelatine, or vortioxetine show stronger evidence than SSRIs for most anhedonic presentations. For treatment-resistant cases, ketamine or TMS may be appropriate. Aerobic exercise supports dopamine recovery, particularly during substance use recovery. Most people improve significantly with a targeted, individualized combination of interventions.
What is an example of anhedonia?
A person who previously loved cooking, listening to music, or spending time with close friends now engages in the same activities but feels nothing. No enjoyment, no anticipation, no satisfaction. The behavior continues but the internal reward signal is absent. A second example is someone in early sobriety who cannot feel pleasure even on objectively positive days, because their dopamine system is still recovering from chronic substance use.
What is the main cause of anhedonia?
The core neurological cause is dopaminergic dysfunction in the reward circuit, specifically reduced activity in the ventral striatum, nucleus accumbens, and prefrontal cortex. At the clinical level, major depressive disorder is the most common cause, followed by substance use disorders, PTSD, schizophrenia, and bipolar disorder. Chronic stress, unresolved trauma, and certain medications including some SSRIs can also suppress reward-circuit function and produce anhedonic symptoms.
When does anhedonia go away?
With treatment, depression-related anhedonia typically improves within 6 to 12 weeks. Substance-related anhedonia in early recovery usually improves over three to twelve months as the dopamine system heals. Trauma-linked anhedonia often persists until trauma-focused therapy addresses the underlying cause. Without treatment, anhedonia rarely resolves on its own. Most people regain the capacity for pleasure with appropriate, sustained clinical care and proper diagnosis.
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Washington, DC: APA; 2013.
- Rømer Thomsen K, et al. “Anhedonia: current and future treatments.” CNS Drugs. 2024.
- Campisi SC, et al. “Anhedonia and Depressive Disorders.” PMC. 2023.
- National Institute of Mental Health. Depression. https://www.nimh.nih.gov/health/topics/depression
- Cleveland Clinic. “Anhedonia.” https://my.clevelandclinic.org/health/symptoms/25155-anhedonia
- WebMD. “Anhedonia: Symptoms, Causes, Treatment.”
- Wikipedia contributors. “Anhedonia.” Wikipedia, The Free Encyclopedia.
